
What the heck is an Aneurysmal Bone Cyst?

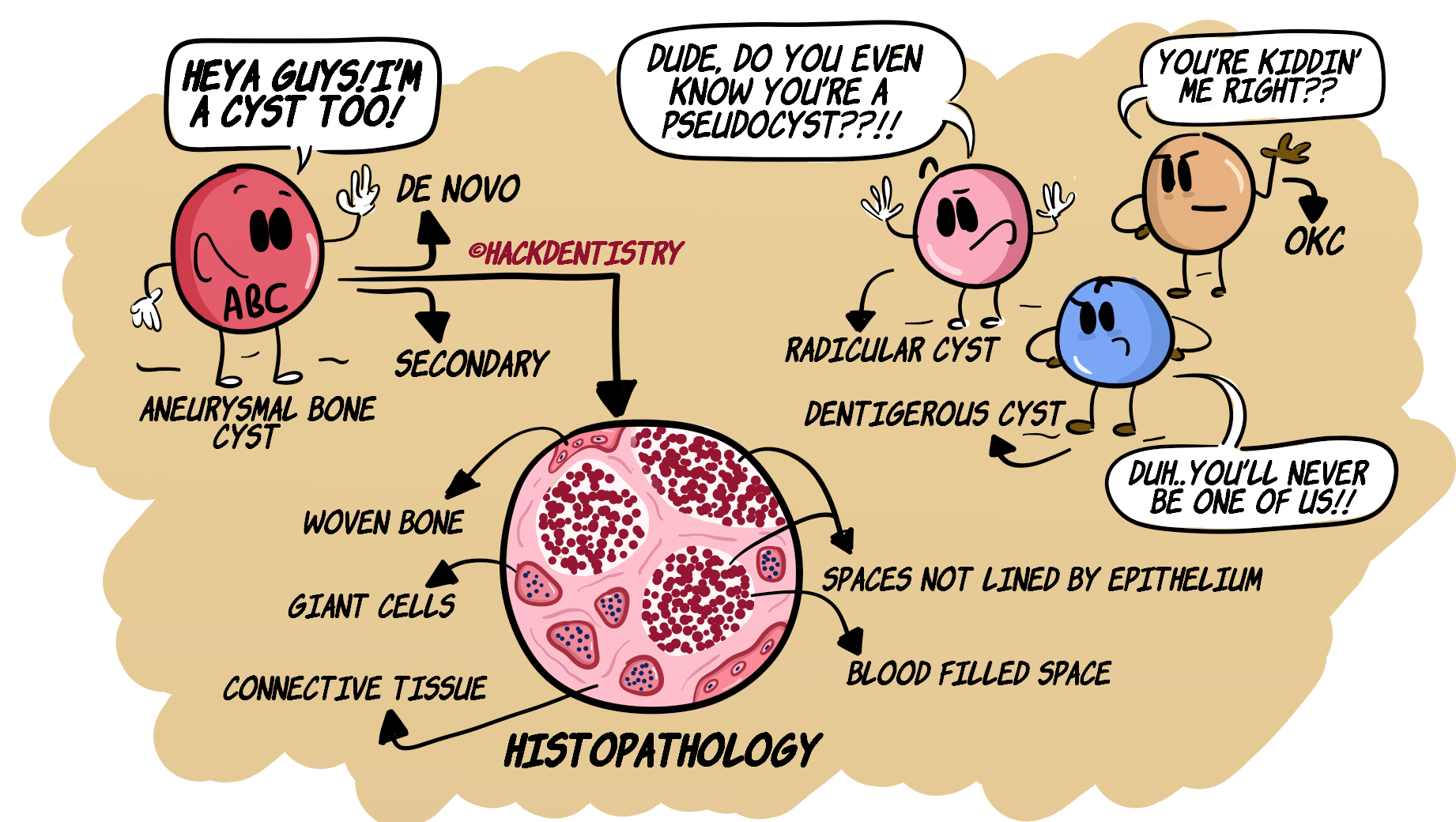
Aneurysmal bone cyst (ABC) is an expansile, osteolytic lesion that consists of blood filled spaces surrounded and separated (a blood filled space from the other) by fibrous connective tissue having multinucleated giant cells and woven bone/osteoid.
This lesion (histologically) has numerous spaces (that are blood filled) --> that mimic cystic spaces. However, since these spaces lack an epithelial lining, ABC is considered to be a pseudocyst.
ABC is considered a) a primary lesion when it arises de novo and b) a secondary lesion when it occurs in association with other lesions.
Some lesions ABC could be secondarily associated with --> central giant cell granuloma (most common), fibro-osseous lesions like fibrous dysplasia and juvenile ossifying fibroma, chondroblastoma, osteosarcoma.
ETIOLOGY & PATHOGENESIS
The etio-pathogenesis for ABC is not clearly known. Many theories have been put forth trying to explain its pathogenesis.
REACTIVE LESION?
Trauma/injury or a primary neoplasm in the bone (central giant cell granuloma, ossifying fibroma, fibrous dysplasia) could initiate a vascular malformation --> local alteration of hemodynamics in the bone --> increased venous pressure --> haemorrhage and resorption of bone --> replacement with connective tissue.
Trauma to bone could possibly cause a hematoma --> failed healing of hematoma --> blood keeps flowing into lesion resulting in accumulation of blood.
NEOPLASTIC LESION?
Chromosomal translocation t(16;17)(q22;p13) --> causes ABC.
Upregulation of oncogene USP6 on chromosome 7p13 --> causes ABC
CLINICAL FEATURES
Bones affected --> a) ABC frequently involves the long bones and vertebrae, b) 12% cases are known to involve bones of the head and neck and c) 2% of ABCs may affect jaw bones.
ABCs occur in the young, usually below 30 years of age. Peak age of incidence --> 2nd decade.
ABC is not known to have any gender predilection.
ORAL MANIFESTATIONS
2/3rds of ABC cases occurring in jaws, affect the mandible --> posterior, molar areas.
ABC usually occurs in the body of the mandible and may extend to the ascending ramus.
There have been rare reports of ABCs occurring in the condyles.
ABC may present as a swelling of the jaw sometimes along with pain.
The lesion is known to cause facial deformity, migration of teeth, malocclusion, cortical thinning, perforation and pathologic fracture.
Maxillary ABCs may cause nasal obstruction, bleeding and proptosis.
RADIOLOGY FEATURES
Usually shows a multilocular, soap bubble appearance.
May also show a unilocular appearance.
Displacement of teeth and root resorption.
Cortical expansion, thinning and perforation.
“Ballooning” or “blow out” expansion of bone (the cortex literally expands like a blown balloon).

HISTOPATHOLOGY FEATURES
The lesion shows numerous blood filled spaces surrounded by a fibro-cellular connective tissue.
The blood filled spaces lack an epithelial lining (pseudo-cystic spaces).
Connective tissue may harbour multinucleated giant cells, numerous fibroblasts and reactive woven bone/osteoid (refer figure in the introduction).
TREATMENT
Intra-operatively, the lesion may appear very bloody --> would look like a “blood soaked sponge”.
Curettage or enucleation would be ideal.
ABC is rarely known to recur but has a good overall prognosis.
✅HIGHLIGHTS - VIVA & ENTRANCE EXAM PERSPECTIVE
ABC (histologically) has numerous blood filled spaces that lack an epithelial lining. Hence ABC is considered to be a pseudocyst.
Some lesions ABC could be secondarily associated with --> central giant cell granuloma (most common), fibro-osseous lesions like fibrous dysplasia and juvenile ossifying fibroma, chondroblastoma, osteosarcoma.
2/3rds of ABC cases occurring in jaws, affect the mandible --> posterior, molar areas.
Radiology --> Usually shows a multilocular, soap bubble appearance.
Radiology --> “Ballooning” or “blow out” expansion of bone (the cortex literally expands like a blown balloon).
Histology --> Blood filled spaces surrounded by connective tissue that harbours multinucleated giant cells, numerous fibroblasts and reactive woven bone/osteoid.
Intra-operatively, the lesion may appear very bloody --> would look like a “blood soaked sponge”
📖REFERENCES AND FURTHER READING
Neville BW, Damm DD, Allen CM, Chi A. Oral and Maxillofacial Pathology. South Asian ed. Elsevier; 2016.
Regezzi JA, Sciubba JJ, Jordan RCK. Oral Pathology: Clinical Pathologic Correlations. 5 th ed. Elsevier; 2007.
Rajendran R, Sivapathasundaram B. Shafer’s Textbook of Oral Pathology. 7th ed. Elsevier; 2012.
Sapp JP, Eversole LR, Wysocki GP. Contemporary Oral and Maxillofacial Pathology. 2 nd ed. Mosby; 2004.