
Cemento-Osseous Dysplasia

Cemento-osseous dysplasia (COD) is a fibro-osseous lesion occurring exclusively in the tooth bearing areas of the jaws.
COD is characterized by the presence of calcifications in the form of spherical masses of cementum-like material and immature woven bone (osteoid) (hence cemento-osseous dysplasia) in a loose fibro-vascular stroma.
💡Controversies with Nomenclature and Origin
The 3rd edition of WHO classification of Head and Neck tumors (2005) renamed this lesion to “osseous dysplasia (OD)” since they contended that bone and cemental tissue cannot be distinguished histologically.
The 4th edition of WHO classification (2017) has reverted to the term “cemento-osseous dysplasia”. Moreover these lesions arise in tooth bearing areas and there is a consensus that it arises from the periodontal ligament. The 4th edition of WHO classification (2017) recognizes three variants of COD --> a) Periapical COD (PCOD), b) Focal COD (FCOD), c) Florid COD (FLCOD).
PCOD and FCOD, are the most common fibro-osseous lesions encountered in clinical practice.
All 3 variants of COD have the same histopathology features and are differentiated based on clinical and radiology features.
💡Know Thy Facts
The term “dysplasia” in cemento-osseous dysplasia, refers to the abnormal/ disordered production and development of bone. It does not refer to or signify the presence of “atypia” or “pre-malignant” features that are described in potentially malignant mucosal lesions like leukoplakia! ETIOLOGY & PATHOGENESIS
There is a general consensus that COD originates from the periodontal ligament (PDL).
This is supported by the fact that a) COD appears in the tooth bearing areas of the jaw, b) histopathology shows the presence of cementum like tissue, c) COD does not appear in other bones in the body (exclusive to jaws).
CLINICAL FEATURES
PERIAPICAL COD (PCOD)
Usually affects middle aged (over 30 years) black females (F:M – 14:1).
It seldom occurs before the age of 20.
PCOD occurs in the periapical areas of mandibular anterior (vital) teeth.
PCOD almost always occurs as multiple lesions (more than 1 lesion).
PCOD is painless/asymptomatic, non-expansile and is usually diagnosed during a radiographic examination.
It could very rarely cause slight expansion of the cortex.
FOCAL COD (FCOD)
Usually affects middle aged black females (F:M – 8:1) in the 4th and 5th decade (mean age of 38 years).
Also reported to affect women of East Asian and Caucasian descent.
Occurs frequently in the mandible in the periapical molar-premolar region (in association with vital tooth).
FCOD could also appear in edentulous areas (usually the mandibular posterior region).
Unlike PCOD, FCOD occurs as a single/isolated lesion.
FCOD is painless/asymptomatic, non-expansile and is usually diagnosed during a radiographic examination.
It could very rarely cause slight expansion of the cortex.
FLORID COD (FLCOD)
Usually affects middle aged to black females in the 4th and 5th decade (mean age of 42 years).
FLCOD has a predilection for the posterior mandible.
Unlike the other two variants of COD, FLCOD usually has a bilateral and almost symmetrical involvement of the mandible.
Rarely, it could involve the maxilla (along with mandible) and affect all 4 quadrants of the jaws.
Usually shows no jaw expansion and may be diagnosed during a radiographic examination.
💡Know Thy Facts
Long standing CODs (all variants) tend to become less vascular and make the affected bone susceptible to infection. This is especially common in FLCOD, where any inflammation due to a periodontal or periapical infection could cause a secondary infection and acute osteomyelitis of the involved bone. In fact, any surgical intervention or extractions of associated teeth are avoided, until necessary. CODs are usually self-limiting and do not require removal. RADIOLOGY FEATURES
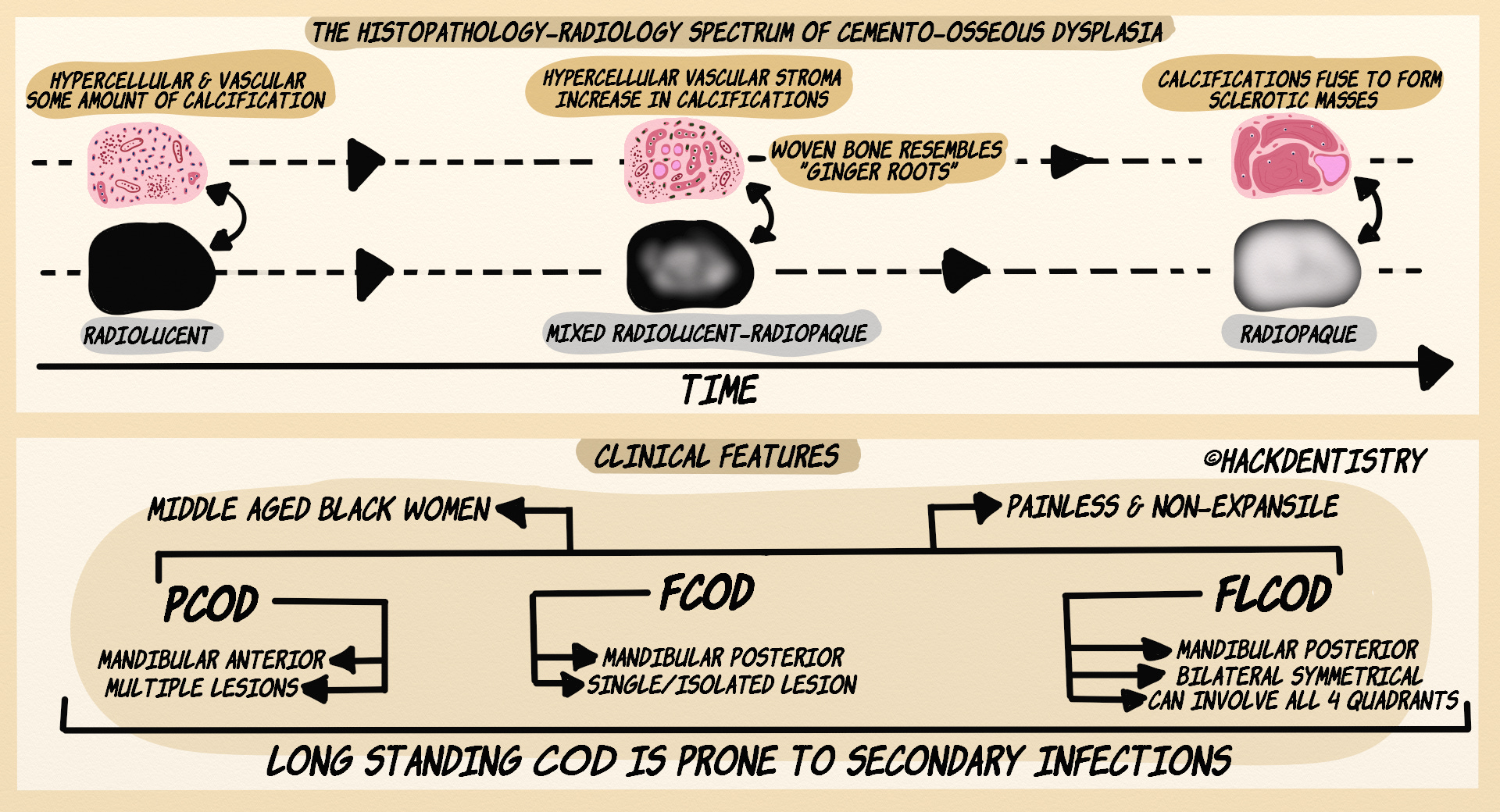
Commonly all variants of COD present as radiolucent lesions in the early stages --> become mixed radiolucent-radiopaque with time --> mature lesions are fully radiopaque.
PCODs (anterior mandible) are usually small seldom growing over 1 cm. Radiolucent PCODs resemble small periapical cysts/granulomas.
FCODs (posterior mandible) are also small lesions, not more than 2 cms in diameter.
PCODs and FCODs are most often mixed radiolucent-radiopaque lesions.
FLCODs appear as multiple confluent (continuous) sclerotic masses in tooth bearing areas, often bilaterally in the mandible.
HISTOPATHOLOGY FEATURES
The histopathology of all variants of COD is similar and indistinguishable.
Initial stage (of the lesion) is characterized by the presence of a loose hypercellular, vascular connective tissue/stroma.
There are numerous small blood vessels and hemorrhage in the connective tissue.
Presence of calcified structures in the connective tissue --> immature bone (osteoid/woven bone) and spherules of cementum-like material.
As the lesion matures,
the stroma becomes less cellular
stroma becomes hypovascular (decrease in blood vessels)
the calcifications (woven bone and cementum like material) increase and become confluent sclerotic masses of tissue.
As the lesion transitions from the initial stages, the woven bone becomes thick and curvilinear resembling “ginger roots”.
TREATMENT
CODs are not neoplastic, do not cause problems. Hence they do not need to be surgically removed.
However, as the lesion matures and becomes hypovascular, the affected bone could be prone to secondary infection, necrosis and osteomyelitis.
Hence, any surgical procedures (for removal of lesion) or extraction of associated teeth should be avoided, lest it may infect the bone.
If secondarily infected, symptomatic treatment and antibiotics are to administered.
✅HIGHLIGHTS - VIVA & ENTRANCE EXAM PERSPECTIVE
Cemento-osseous dysplasia (COD) is a fibro-osseous lesion occurring exclusively in the tooth bearing areas of the jaws.
The 4th edition of WHO classification (2017) recognizes three variants of COD --> a) Periapical COD (PCOD), b) Focal COD (FCOD), c) Florid COD (FLCOD).
All 3 variants of COD basically have the same histopathology features and are differentiated based on clinical and radiology features.
There is a general consensus that COD originates from the periodontal ligament (PDL).
All variants of COD predominantly affect middle aged black females.
PCOD almost always occurs as multiple lesions in the mandibular anterior periapical region.
FCOD occurs as a single, isolated lesion in the mandibular molar-premolar region.
Unlike the other two variants of COD, FLCOD usually has a bilateral, almost symmetrical involvement of the mandible and could also rarely involve the maxilla affecting all 4 quadrants.
Commonly all variants of COD present as radiolucent lesions in the early stages --> become mixed radiolucent-radiopaque with time --> mature lesions are fully radiopaque.
Initial stage (of the lesion) is characterized by the presence of a loose hypercellular, vascular connective tissue/stroma.
Presence of calcified structures in the connective tissue --> immature bone (osteoid/woven bone) and spherules of cementum-like material.
As the lesion transitions from the initial stages, the woven bone becomes thick and curvilinear resembling “ginger roots”.
📖REFERENCES AND FURTHER READING
Neville BW, Damm DD, Allen CM, Chi A. Oral and Maxillofacial Pathology. South Asian ed. Elsevier; 2016.
Regezzi JA, Sciubba JJ, Jordan RCK. Oral Pathology: Clinical Pathologic Correlations. 5 th ed. Elsevier; 2007.
Wood NK, Goaz PW. Differential Diagnosis of Oral and Maxillofacial Lesions. 5 th ed. Mosby; 1997.