
Cemento-Ossifying Fibroma (Notes & Video)

💡Before you start…
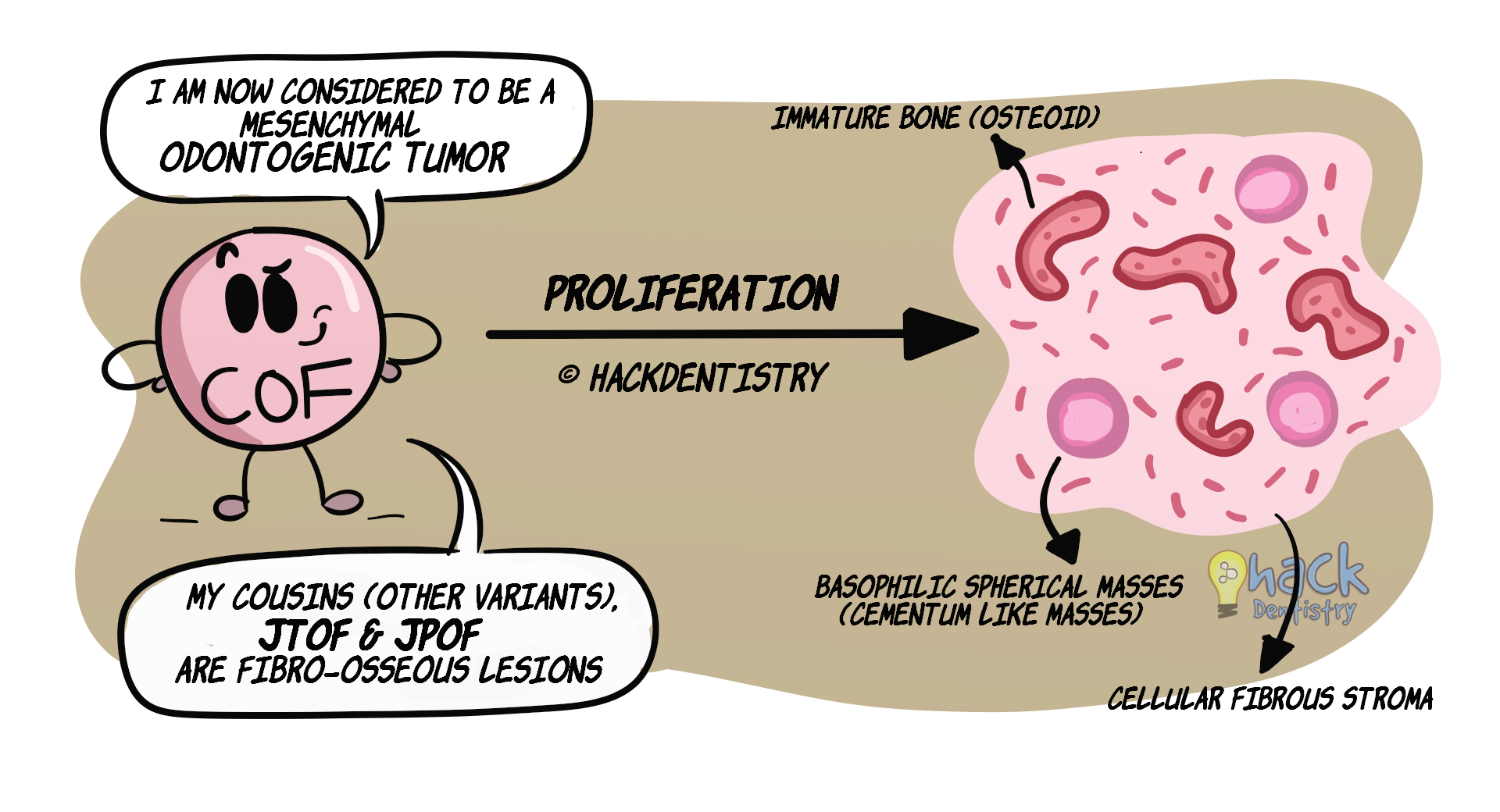
This video was made before the recent updates and classification of cemento-ossifying fibroma(COF). COF was previously called ossifying fibroma and is now considered to be a mesenchymal odontogenic tumor. Refer the notes for the recent updates. Otherwise the clinical features, radiology and histopathology for the lesion remain the same. Cemento-ossifying fibroma (COF) is a tumor where there is proliferation of cellular (fibroblasts) fibrous tissue along with calcifications in the form of basophilic spherical masses (cementum-like material) & immature bone (osteoid) (hence cemento-ossifying fibroma).
COF is a true neoplasm, in that, it has a proliferative (growth) potential and can cause expansion of bone.
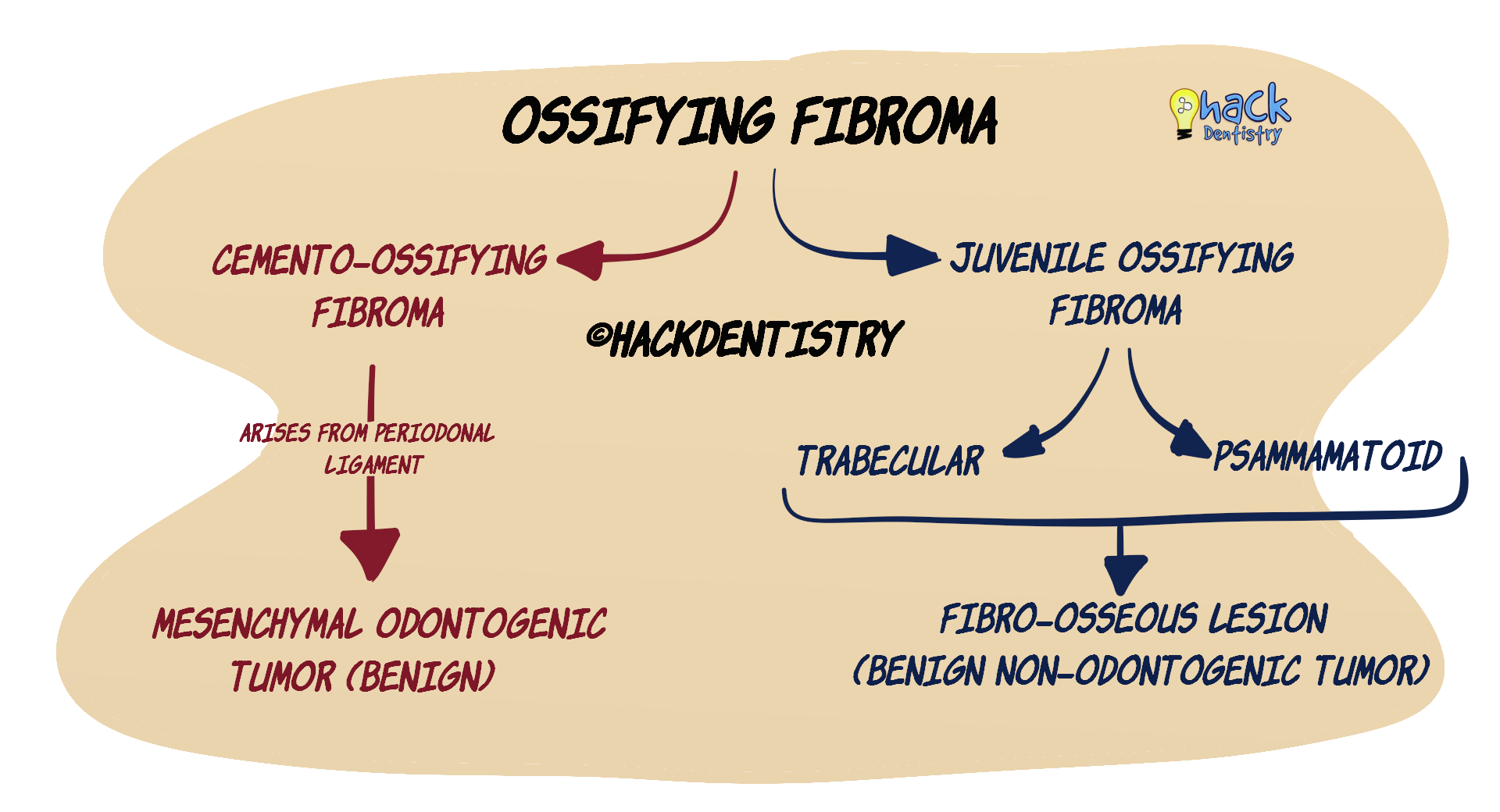
The most recent (2017) WHO classification considers ossifying fibroma (OF) in general to have three variants --> a) COF, considered to be odontogenic in origin, and non-odontogenic variants called b) juvenile trabecular OF (JTOF), c) juvenile psammamatoid OF(JPOF) (refer Figure 1).
MOST RECENT CLASSIFICATION OF OSSIFYING FIBROMA
📖Sources
- Speight PM, Takata T. New tumour entities in the 4th edition of the World Health Organization Classification of Head and Neck tumours: odontogenic and maxillofacial bone tumours. Virchows Arch. 2018 Mar;472(3):331-339.
- El-Mofty SK. Fibro-osseous lesions of the craniofacial skeleton: an update. Head Neck Pathol.2014 ;8(4):432–444. PATHOGENESIS
Sporadic cases (not all lesions) of COF have a mutation in the HRPT2 gene that encodes for the parafibromin protein.
COF is thought to arise from the progenitor cells in the periodontal ligament.
💡CONTROVERSIES WITH NOMENCLATURE & ORIGIN
The problem with nomenclature and origin (odontogenic or fibro-osseous) of COF has always been a controversy due to the presence of both “immature bone (osteoid)” and “basophilic spherical cementum-like calcifications” (since they resemble cementicles).
- The 2nd edition of WHO classification of Head & Neck Tumors (1992) termed this lesion as “cemento-ossifying fibroma”.
- The 3rd edition of WHO classification (2005) renamed the lesion to “ossifying fibroma (OF)” since they contended that bone and cemental tissue cannot be distinguished histologically. Moreover OF has variants (juvenile [trabecular & psammamatoid] OF) arising in non-tooth associated regions (paranasal sinuses) (This is explained in the video in detail. You can watch it to understand the controversies better. But the video was done prior to the most recent updates being released).
- The 4th edition of WHO classification (2017) felt that the term “cemento-ossifying fibroma” is descriptive of the lesion. Moreover these lesions arise in tooth bearing areas (usually mandibular molar-premolar areas) and there is a consensus that it is odontogenic in origin (from periodontal ligament). Other variants (juvenile [trabecular & psammamatoid] OF) are termed “ossifying fibromas” and are considered to be fibro-osseous lesions (non-odontogenic). CLINICAL FEATURES
COF has a female predilection and usually occurs in the 3rd to 4th decades of life.
It has a predilection for the mandibular premolar-molar area (usually molar).
COF is a slow growing, expansive (buccal or lingual expansion) lesion and could clinically cause swelling and facial asymmetry.
COF is centrifugal in growth, meaning it maintains its round or oval shape on enlargement.
The centrifugal growth pattern may cause a bowing (downward expansion) of the inferior border of the mandible.
COFs could rarely be small lesions, not causing an expansion. Such lesions are diagnosed during a routine radiographic examination.
RADIOLOGY FEATURES
Well circumscribed lesion with a sclerotic border.
The lesion may appear radiolucent initially and with time becomes mixed radiolucent-radiopaque.
End stage lesions may be completely radiopaque.
Large lesions may show downward bowing of inferior border of mandible.
May show root resorption and displacement of surrounding teeth.
HISTOPATHOLOGY FEATURES
Hypercellular connective tissue with numerous fibroblasts (often) arranged in a storiform pattern.
Presence of calcified structures in the connective tissue --> immature bone (osteoid/woven bone) and basophilic spherules of cementum-like material.
Either of the calcified tissues (osteoid or cementum-like material) could dominate in different cases (ratios of these calcified structures may vary).
The immature bone (osteoid/woven bone) may be lined by osteoblasts -> called osteoblastic rimming.
TREATMENT
Complete surgical excision.
Usually shells/enucleates out as a whole, intact mass.
Has a good prognosis.
💡A NOTE ON (JUVENILE) VARIANTS OF OSSIFYING FIBROMA
Other than COF, ossifying fibroma (OF) has two other non-odontogenic variants called juvenile trabecular OF (JTOF) and juvenile psammamatoid OF (JPOF).
JTOF
JTOF usually occurs in children in the age group of 8.5-12 years.
Most frequently affects the maxilla and could show rapid expansion.
May cause blockade of nasal passages and epistaxis.
Mixed-radiolucent-radiopaque appearance.
Histopathology --> Hypercellular stroma (fibroblasts), presence of immature bony (osteoid) trabeculae, presence of osteoclastic giant cells.
JPOF
Occurs in the young; age range --> 16 – 33 years.
Occurs in extragnathic sites --> paranasal sinuses, orbit, nasal bones.
May cause sinusitis, proptosis, nasal obstruction and blindness.
Round, well defined osteolytic lesion; may show ground glass appearance.
Histopathology --> Hypercellular stroma (fibroblasts), presence of round “ossicles” that resemble psammoma bodies (hence the name for this variant).
✅HIGHLIGHTS - VIVA & ENTRANCE EXAM PERSPECTIVE
Cemento-ossifying fibroma (COF) is a tumor where there is proliferation of cellular (fibroblasts) fibrous tissue along with calcifications in the form of basophilic spherical masses (cementum-like material) & immature bone (osteoid) (hence cemento-ossifying fibroma).
The most recent (2017) WHO classification considers ossifying fibroma (OF) in general to have three variants --> a) COF, considered to be odontogenic in origin, and non-odontogenic variants called b) juvenile trabecular OF (JTOF), c) juvenile psammamatoid OF(JPOF)
COF is thought to arise from the progenitor cells in the periodontal ligament.
COF has a female predilection and usually occurs in the 3rd to 4th decades of life.
It has a predilection for the mandibular premolar-molar area (usually molar).
COF is centrifugal in growth, meaning it maintains its round or oval shape on enlargement
The centrifugal growth pattern of COF may cause a bowing (downward expansion) of the inferior border of the mandible.
The lesion may appear radiolucent initially and with time becomes mixed radiolucent-radiopaque.
Histopathology --> Presence of calcified structures in the connective tissue -> immature bone (osteoid/woven bone) and basophilic spherules of cementum-like material.
JTOF most frequently affects the maxilla and could show rapid expansion.
JPOF ccurs in extragnathic sites --> paranasal sinuses, orbit, nasal bones.
📖REFERENCES AND FURTHER READING
Barnes L, Eveson JW, Reichart P, Sidransky D (2005) Odontogenic Tumours. Ch 6, WHO classification of tumors: pathology and genetics of head and neck tumours. IARC, Lyon.
Neville BW, Damm DD, Allen CM, Chi A. Oral and Maxillofacial Pathology. South Asian ed. Elsevier; 2016.
Regezzi JA, Sciubba JJ, Jordan RCK. Oral Pathology: Clinical Pathologic Correlations. 5 th ed. Elsevier; 2007.
Wood NK, Goaz PW. Differential Diagnosis of Oral and Maxillofacial Lesions. 5 th ed. Mosby; 1997.