
Central giant cell granuloma (Notes & Video)

Central giant cell granuloma (CGCG) is a benign osteolytic lesion of the bone, predominantly affecting the jaws.
First described by Jaffe in 1953, CGCG was thought to be a reactive response to intra-bony hemorrhage. It was then called “Giant cell reparative granuloma”.
However, CGCG occasionally exhibits aggressive behaviour and is also thought to be related to its aggressive long bone counterpart - Giant cell tumor (GCT).
Hence many researchers and pathologists consider CGCG to be a benign neoplasm.
ETIOLOGY & PATHOGENESIS
The etiology for CGCG is unknown, although there are sporadic cases which show a genetic cause.
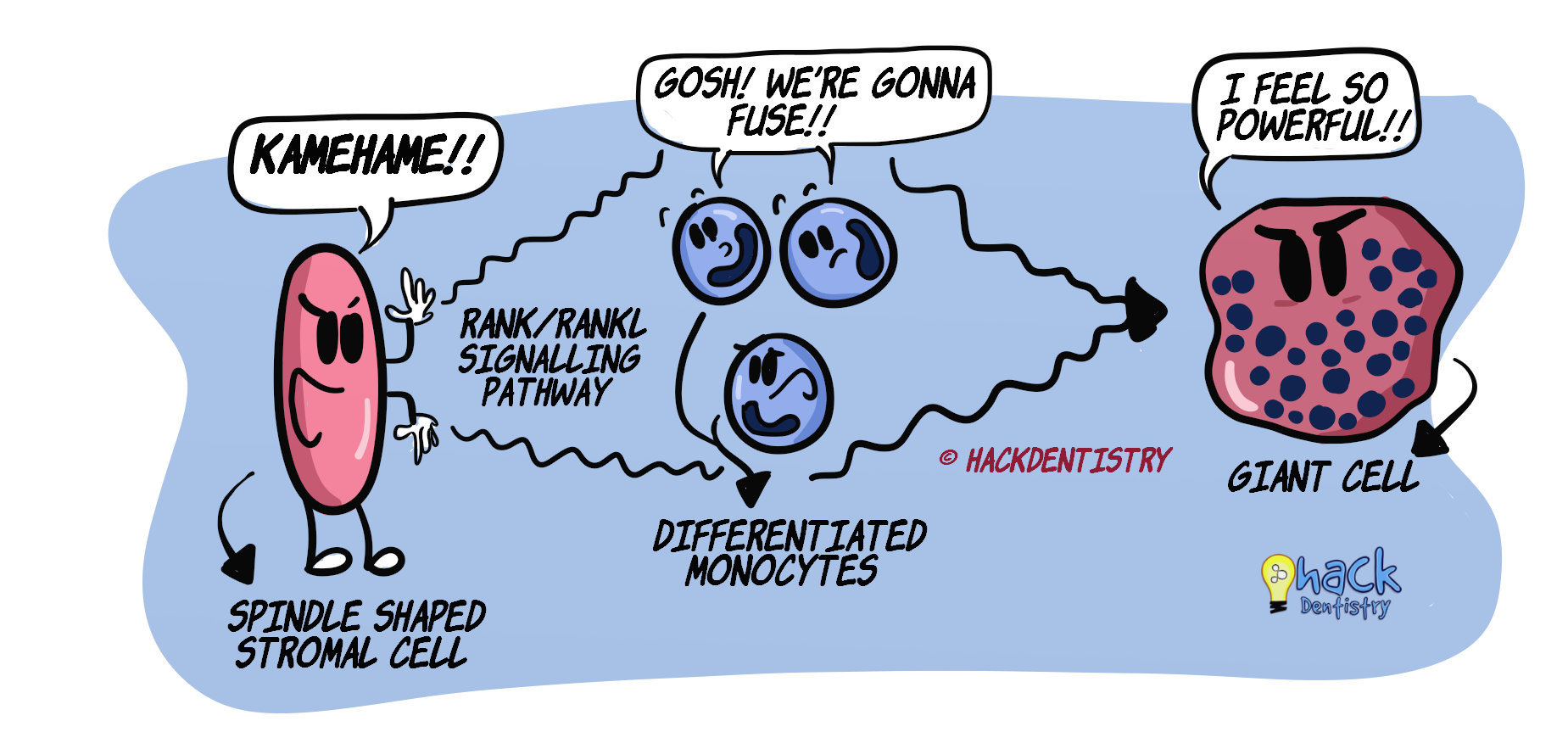
Two important types of cells that play major roles in this disease process are a) spindle shaped stromal cells (SSCs) and b) multinucleate giant cells.
SSCs form the proliferative component. These are “osteoblast-like” cells, since they express many osteoblastic proteins like RANK ligand (RANKL), alkaline phosphatase and many others.
SSCs recruit monocytes from blood (to the lesional site)

SSCs help these recruited monocytes differentiate into “osteoclast-like” precursors expressing RANK receptors

SSCs, through RANK/RANKL signalling pathway, induce the fusion of these (differentiated) monocytes to form multinucleated giant cells
CLINICAL FEATURES
CGCG has a female predilection and usually occurs in the young, below 30 years.
The lesion prefers the mandible and occurs most frequently in front of the molars, usually the anteriors.
The lesion is known to cross the midline, meaning extending from one quadrant to another (for example – from mandibular left canine --> crosses the midline --> extends up to the mandibular right canine).
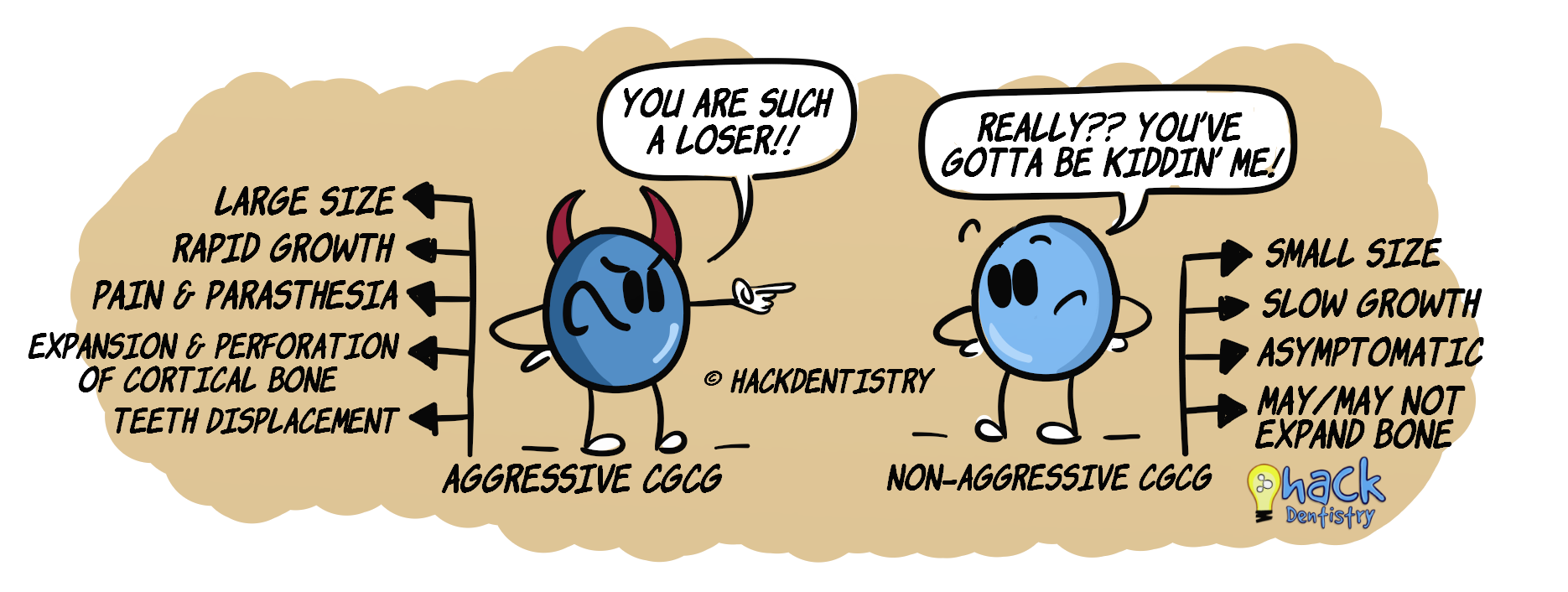
CGCG is known to be of two types depending on its clinico-radiologic profile --> a) Non-aggressive type (more frequent) b) Aggressive type
NON-AGGRESSIVE TYPE
Most cases of CGCG are non-aggressive.
They a) are small in size, b) show slow growth, c) are asymptomatic (no pain), and d) may or may not show bony expansion
The non-aggressive CGCG may at times be diagnosed only during routine radiographic examination.
AGGRESSIVE TYPE
Sometimes CGCG may show aggressive & destructive behaviour.
These lesions a) are large in size, b) show rapid growth, c) may cause pain and paraesthesia, d) cause cortical expansion, thinning and perforation, and e) displacement of teeth and resorption of roots.
Aggressive lesions have a high recurrence rate.
KNOW THY FACTS!
CGCG is an osteolytic bone lesion that is mostly confined to the jaws. Very rarely, it may involve other bones in the craniofacial complex and the bones of the hands and feet.
There are rare reported cases of multiple CGCGs appearing at a time. Such cases are usually associated with syndromes like Noonan syndrome or Neurofibromatosis type 1.
RADIOLOGY FEATURES
Non-aggressive lesions -> unilocular appearance
Aggressive lesions --> multilocular appearance, root resorption, cortical thinning/perforation, displacement of teeth.
HISTOPATHOLOGY FEATURES
The lesion shows a loose fibrous stroma with a high vascular density --> numerous blood vessels (capillaries).
Two important cells to note in the stroma --> a) spindle shaped stromal cells (these are mononuclear cells that are spindle shaped, resemble fibroblasts) and b) multinucleate giant cells.
Giant cells vary in size --> number of nuclei ranging from a few to many dozen.
Focal areas in the stroma may be hemorrhagic with lots of extravasated red blood cells.
Periphery of the lesion may show focal areas of osteoid/immature bone formation.
TREATMENT
Complete surgical enucleation.
Aggressive lesions are treated with an en-bloc resection to minimize recurrence.
Non-surgical modes of treatment --> administration of corticosteroid injections, calcitonin, interferon-α.
HIGHLIGHTS - VIVA & ENTRANCE EXAM PERSPECTIVE
Two important types of cells that play major roles in disease process of central giant cell granuloma (CGCG) are a) spindle shaped stromal cells (SSCs) and b) multinucleate giant cells.
Spindle shaped stromal cells form the proliferative component. These are “osteoblast-like” cells, since they express many osteoblastic proteins.
CGCG prefers the mandible and occurs most frequently in front of the molars, usually the anteriors.
CGCG is known to cross the midline, meaning extending from one quadrant to another (for example – from mandibular left canine --> crosses the midline --> extends up to the mandibular right canine).
Most cases of CGCG are non-aggressive.
Aggressive CGCGs a) are large in size, b) show rapid growth, c) may cause pain and paraesthesia, d) cause cortical expansion, thinning and perforation, and e) displacement of teeth and resorption of roots.
Two important cells to note in the stroma (microscopy) --> a) spindle shaped stromal cells (these are just mononuclear cells that are spindle shaped, resemble fibroblasts) and b) multinucleate giant cells.
REFERENCES AND FURTHER READING
Cowan RW, Singh G. Giant cell tumor of bone: a basic science perspective. Bone. 2013;52(1):238-46.
Hosur MB, Puranik RS, Vanaki SS, Puranik SR, Ingaleshwar PS. Clinicopathological profile of central giant cell granulomas: An institutional experience and study of immunohistochemistry expression of p63 in central giant cell granuloma. J Oral Maxillofac Pathol. 2018;22(2):173–179.
Chrcanovic BR, Gomes CC, Gomez RS. Central giant cell lesion of the jaws: An updated analysis of 2270 cases reported in the literature. J Oral Pathol Med. 2018 Sep;47(8):731-739.
de Lange J, van den Akker HP, van den Berg H. Central giant cell granuloma of the jaw: a review of the literature with emphasis on therapy options. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104(5):603-15.
Neville BW, Damm DD, Allen CM, Chi A. Oral and Maxillofacial Pathology. South Asian ed. Elsevier; 2016.
Regezzi JA, Sciubba JJ, Jordan RCK. Oral Pathology: Clinical Pathologic Correlations. 5 th ed. Elsevier; 2007.
Rajendran R, Sivapathasundaram B. Shafer’s Textbook of Oral Pathology. 7th ed. Elsevier; 2012.