
Cherubism

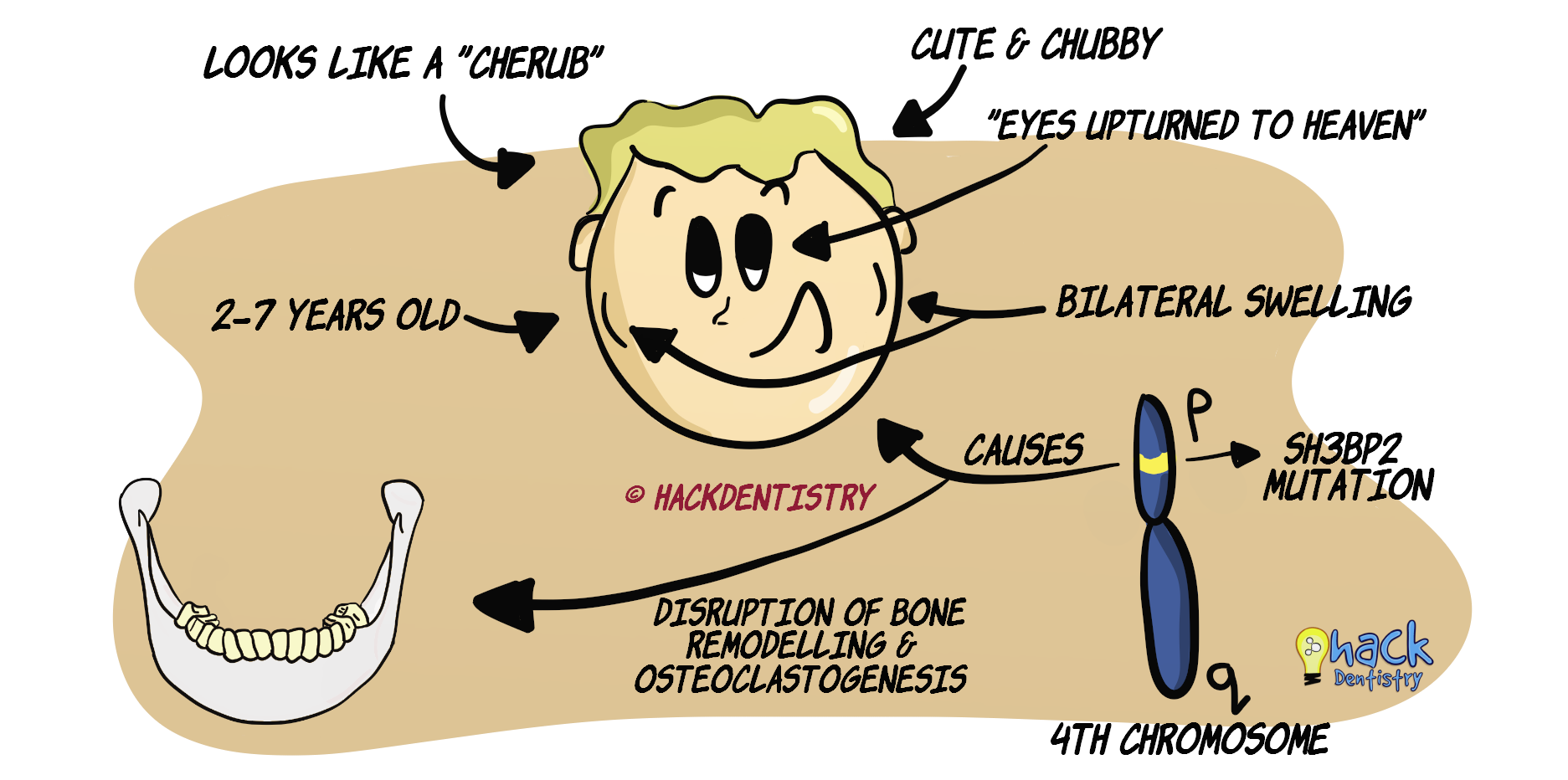
Cherubism is a hereditary, developmental condition that causes bilateral, symmetrical swelling of the jaws affecting children usually between 2-7 years.
The bilateral swelling produces a plump cheeked, chubby look resembling little angels called “cherubs”, hence the name “cherubism”.
💡Know Thy Facts
Cherubism was also called “familial fibrous dysplasia (FFD)”. However, it has to be noted that, cherubism is a totally different entity and has no relation to fibrous dysplasia. Hence the usage of the term FFD is better avoided. ETIOLOGY & PATHOGENESIS
Cherubism is inherited as an autosomal dominant trait, although there have been rare reports of sporadic cases with no hereditary mutation.
The mutation has been mapped to the SH3BP2 gene on chromosome 4p16.
This mutation is known to disrupt normal bone remodelling and upregulate osteoclastogenesis.
Inflammation is also hypothesized to play a role in this condition.
Inflammation along with excessive osteoclastic activity causes multilocular bone resorptions in the jaw filled with fibrous tissue.
The dysplastic fibrous tissue grows within and expands the bone, causing swelling of the jaws (bilaterally) giving a chubby look.
Cherubism is known to have a 100% penetrance in males and 50-75% penetrance in females.
CLINICAL FEATURES
Cherubism is evident in children usually within 2-7 years.
The most usual sign is a bilateral symmetric swelling of the posterior mandible.
Submandibular and cervical lymphadenopathy also contributes to the fullness of the face and is a fairly common manifestation.
There have been rare cases of unilateral involvement of the jaw.
The lesion continues to progress up to puberty, at which point it stops growing and begins to regress afterwards.
Signs and symptoms of cherubism vary and may range from being a mild bilateral swelling, to a severe swelling resulting in functional impairment like mastication and speech.
“Eyes upturned to heaven” appearance --> this is a result of the lesion involving the inferior and lateral orbital bone, titling the eyeballs upwards and retracting the lower eyelids. This exposes the sclera thereby giving this appearance.
BONES (JAWS) INVOLVED
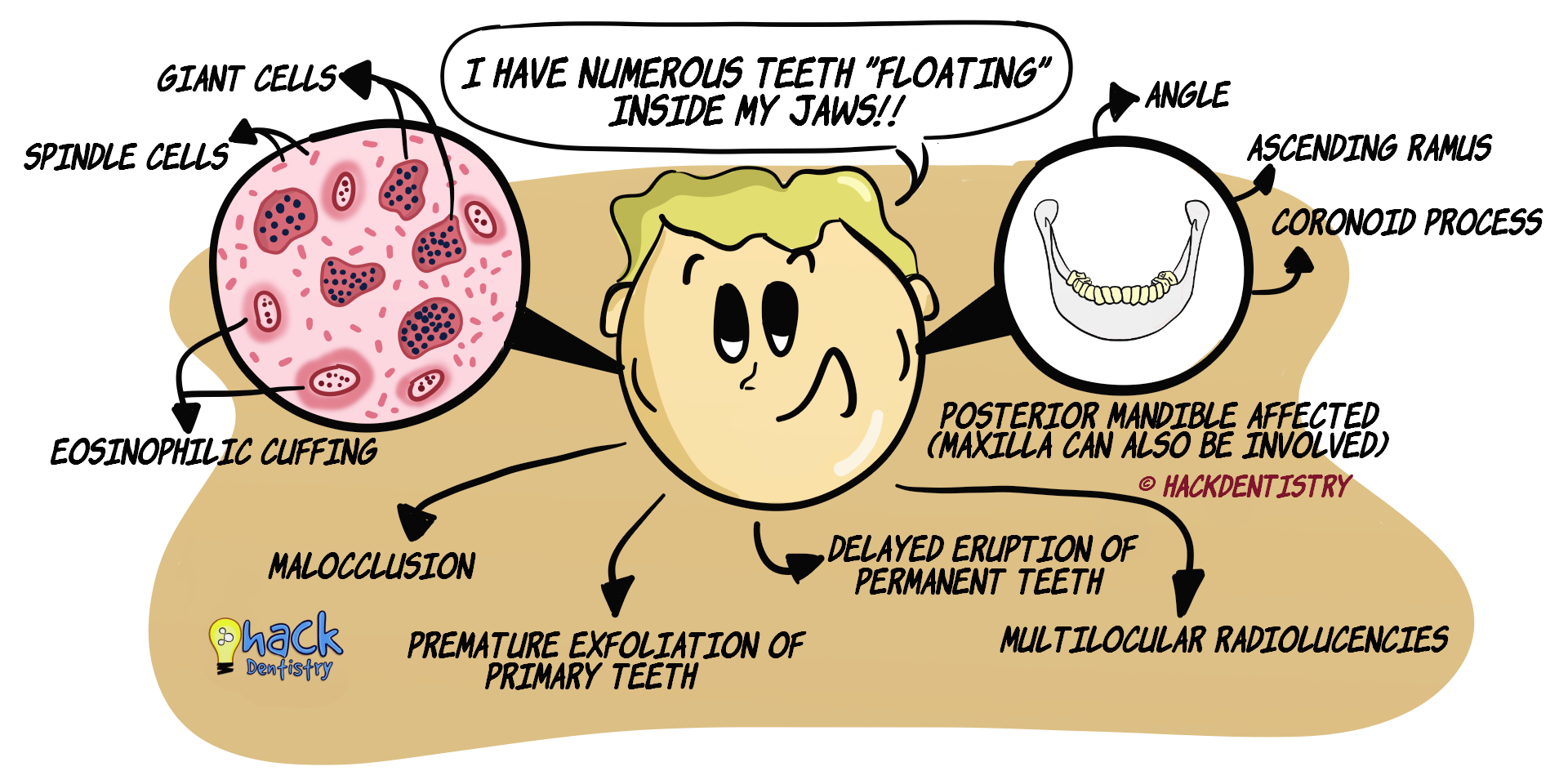
Cherubism mostly involves the posterior mandible --> angles, ascending rami and coronoid processes. The condyles are mostly not affected.
Severe cases may also involve the maxilla (along with the mandible) --> either only the tuberosities or the whole of maxilla.
GRADING OF CHERUBISM
One of the first grading system used to describe cherubism ranked it in three grades according to the extent of involvement of the jaws.
Grade I - Bilateral symmetrical expansion of mandibular rami
Grade II - Involvement of rami and body of mandible together with maxillary tuberosities.
Grade III – Involvement of the entire mandible and maxilla along with considerable facial deformity.
There have been other grading systems also proposed (refer 6th article in reference section).
ORAL/DENTAL COMPLICATIONS
Widening of alveolar ridges.
Narrow, V-shaped maxillary arch (if the maxilla is involved).
Displacement of teeth leading to malocclusion.
Mobility of teeth.
Premature exfoliation of primary teeth.
Delayed eruption of permanent teeth.
Impaired mastication and speech problems.
In severe cases swelling of both mandible and maxilla could cause a backward displacement of the tongue leading to airway obstruction.
RADIOLOGY FEATURES
Bilateral multilocular radiolucencies of the mandible and/or maxilla.
Thinning and perforation of cortical bone.
Displacement of teeth and resorption of roots.
Numerous unerupted teeth appear to be “floating” within the jaws.
Displacement of inferior alveolar canal
HISTOPATHOLOGY FEATURES
Histopathology shows resemblance to central giant cell granuloma.
The lesion shows a vascular loose fibrous stroma.
Presence of spindle cells and giant cells in stroma.
A characteristic feature of cherubism is the presence an eosinophilic material around blood vessels. This is called “eosinophilic cuffing”.
TREATMENT
Usually no treatment is warranted for mild cases, especially if the lesion only involves the mandible.
The condition is self-limiting, starts to regress after puberty and resolves within the third decade.
In severe cases where there may be functional and esthetic problems, surgical intervention in the form of curettage, resection and bone contouring can be done.
✅HIGHLIGHTS - VIVA & ENTRANCE EXAM PERSPECTIVE
Cherubism is a hereditary, developmental condition that causes bilateral, symmetrical swelling of the jaws affecting children usually between 2-7 years.
Cherubism was also called “familial fibrous dysplasia (FFD)”. However, it has to be noted that, cherubism is a totally different entity and has no relation to fibrous dysplasia. Hence the usage of the term FFD is better avoided.
Cherubism is inherited as an autosomal dominant trait, with the mutation being mapped to the SH3BP2 gene on chromosome 4p16.
The most usual sign is a bilateral symmetric swelling of the posterior mandible.
“Eyes upturned to heaven” appearance --> this is a result of the lesion involving the inferior and lateral orbital bone, titling the eyeballs upwards. This exposes the sclera thereby giving this appearance.
Cherubism mostly involves the posterior mandible --> angles, ascending rami and coronoid processes. The condyles are mostly, not affected.
Oral complications --> premature exfoliation of primary teeth & delayed eruption of permanent teeth.
Bilateral multilocular radiolucencies of the mandible and/or maxilla.
Numerous unerupted teeth appear to be “floating” within the jaws.
Histopathology shows resemblance to central giant cell granuloma.
📖REFERENCES AND FURTHER READING
Kannu P, Baskin B, Bowdin S. Cherubism. 2007 Feb 26 [Updated 2018 Nov 21]. In: Adam MP, Ardinger HH, Pagon RA, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2019.
Degala S, Mahesh KP, Monalisha. Cherubism: a case report. J Maxillofac Oral Surg.2015;14(Suppl 1):258–262.
Kömerik N, Taş B, Önal L. Cherubism. Head Neck Pathol.2014;8(2): 164–167.
Papadaki ME, Lietman SA, Levine MA, Olsen BR, Kaban LB, Reichenberger EJ. Cherubism: best clinical practice. Orphanet J Rare Dis. 2012;7 Suppl 1(Suppl 1):S6. doi:10.1186/1750-1172-7-S1-S6.
Neville BW, Damm DD, Allen CM, Chi A. Oral and Maxillofacial Pathology. South Asian ed. Elsevier; 2016.
Regezzi JA, Sciubba JJ, Jordan RCK. Oral Pathology: Clinical Pathologic Correlations. 5 th ed. Elsevier; 2007.
Rajendran R, Sivapathasundaram B. Shafer’s Textbook of Oral Pathology. 7th ed. Elsevier; 2012.