
Dentigerous & Eruption cyst (Note & Video)

Dentigerous cyst is the most common “developmental” odontogenic cyst. It makes up 20% of all jaw cysts occurring in the oral cavity.
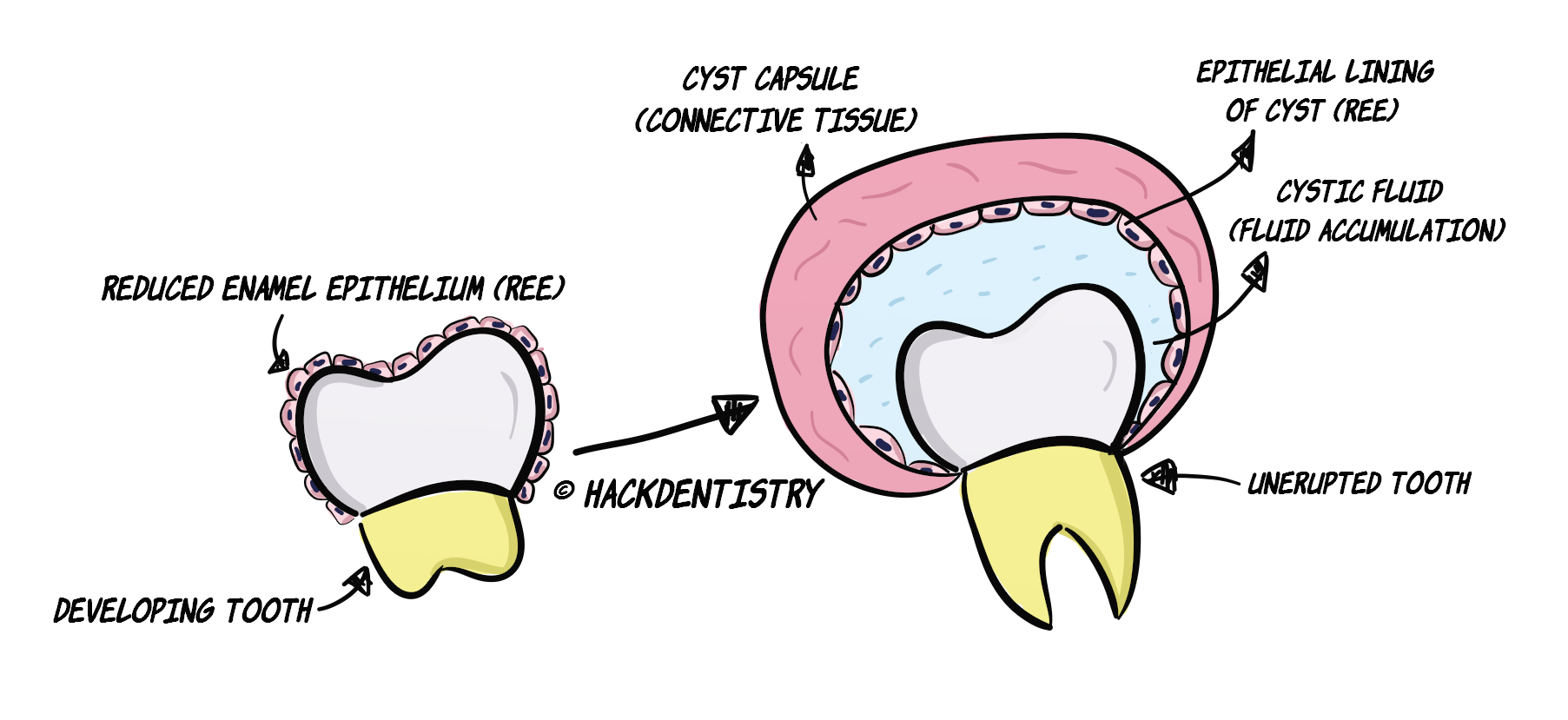
This cyst develops as a result of fluid accumulation between the reduced enamel epithelium and the enamel surface of the developing tooth.
This results in a cyst enclosing the crown and is attached to the cement-enamel junction of the tooth.
Remember that radicular/periapical cyst is the most common odontogenic cyst occurring in the oral cavity (50-60% of all jaw cysts). It however, is an inflammatory cyst (inflammatory in origin; dentigerous cyst is developmental in origin). Dentigerous cyst is the 2nd most common (next to radicular cyst) odontogenic cyst, but most common "developmental" odontogenic cyst.CLINICAL FEATURES
Dentigerous cyst predominantly occurs between the second and third decades of life (10-30 years).
Has a slight male predilection.
It is associated with an unerupted tooth, usually the mandibular 3rd molar (65%).
Most common teeth affected --> mandibular 3rd molar > maxillary cuspid > maxillary 3rd molar > mandibular 2nd premolar.
Dentigerous cyst may also be rarely associated with a supernumerary tooth or an odontome.
This cyst is usually asymptomatic and is discovered in radiographs. May also grow to large sizes causing sufficient swelling and facial asymmetry.
RADIOLOGY FEATURES
Dentigerous cyst shows a pericoronal radiolucency i.e a unilocular radiolucency around the crown of the tooth. The radiolucency usually confines itself upto the CEJ of the tooth.
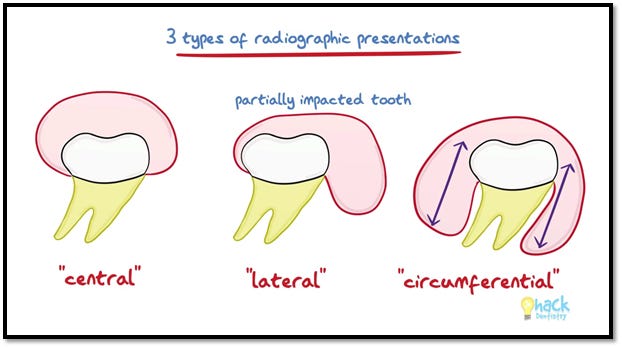
There are three radiographic varieties of dentigerous cyst --> a) Central, b) Lateral and c) Circumferential.
Central --> Most common variety. Radiolucency surrounds the crown and extends upto CEJ of tooth
Lateral -> Radiolucency may extend laterally along the root and partially surround the crown.
Circumferential --> Radiolucency extends along the roots and appears to cover the root.
The diameter of the radiolucency surrounding the crown has to be greater than 3-4 mm or at least 5mm for consideration of a diagnosis of dentigerous cyst. Otherwise, it could be an enlarged follicular space.
( *Neville BW, Damm DD, Allen CM, Chi A. Oral and Maxillofacial Pathology, quotes 3-4mm to be ideal for diagnosis, while Rajendran R, Sivapathasundaram B. Shafer’s Textbook of Oral Pathology, quotes a space >5mm to be necessary for a diagnosis.)
💡CAUTION!
A suspect diagnosis of a large dentigerous cyst (made with a radiographic examination) could be considered otherwise. Dentigerous cyst is usually small, and large lesions may turn out to be other odontogenic cysts or tumors mimicking dentigerous cyst.
Some lesions mimicking dentigerous cyst in the radiograph (pericoronal radiolucency):
- Unicystic ameloblastoma
- Conventional ameloblastoma
- Adenomatoid odontogenic tumor
- Odontogenic keratocyst
- Ameloblastic fibroma
- Calcifying epithelial odontogenic tumor (rarely)HISTOPATHOLOGY FEATURES
2-4 layers of flattened non-keratinized odontogenic epithelium lining a loosely fibrous connective tissue.
The epithelium may be flat or cuboidal and essentially represents the reduced enamel epithelium.
The connective tissue may harbour small islands or cords of odontogenic epithelium.
💡POTENTIAL COMPLICATIONS
The epithelial lining of dentigerous cyst may potentially undergo a neoplastic transformation and give rise to complications like a) ameloblastoma, b) squamous cell carcinoma and c) mucoepidermoid carcinoma. The possibility of these lesions arising from the dentigerous cyst are however, very rare.TREATMENT
Dentigerous cyst is usually treated by enucleation along with removal of involved tooth.
Large cysts can be treated by marsupialization.
💡ERUPTION CYST: A BRIEF NOTE
Eruption cyst also called eruption hematoma is the soft tissue variant of dentigerous cyst.
The pathogenesis of eruption cyst is the same as dentigerous cyst except that the (in the case of eruption cyst) eruption of the associated tooth is impeded in the soft tissue. The cyst comes to surround the tooth in the soft tissue.
Appears as a blue to purple, small fluctuant and translucent swelling on the alveolar ridge on the site of the erupting tooth.
Usually seen in children younger than 10 years.
Teeth most commonly associated with --> deciduous mandibular central incisor > mandibular 1st permanent molars > deciduous maxillary incisor.
QUESTIONS? BRING ‘EM ON!!
Would dentigerous cyst show its characteristic histopathology picture if it was infected/inflamed?
ANSWER
It wouldn’t! An inflamed dentigerous cyst would show moderate to dense inflammation of the connective tissue. The connective tissue would also become more collagenous/fibrous. Also the epithelium may become hyperplastic, and develop rete ridges.
✅HIGHLIGHTS - VIVA & ENTRANCE EXAM PERSPECTIVE
Dentigerous cyst is the most common developmental odontogenic cyst.
This cyst develops as a result of fluid accumulation between the reduced enamel epithelium and the enamel surface of the developing tooth.
Dentigerous cyst predominantly occurs between the second and third decades of life (10-30 years).
Most common teeth affected --> mandibular 3rd molar > maxillary cuspid > maxillary 3rd molar > mandibular 2nd premolar.
There are three radiographic varieties of dentigerous cyst --> a) Central, b) Lateral and c) Circumferential.
The diameter of the radiolucency surrounding the crown has to be greater than 3-4 mm for consideration of a diagnosis of dentigerous cyst.
A suspect diagnosis of a large dentigerous cyst (made with a radiographic examination) should be considered otherwise. Dentigerous cyst is usually small, and large lesions may turn out to be other odontogenic cysts or tumors mimicking dentigerous cysts.
The epithelial lining of dentigerous cyst may potentially undergo a neoplastic transformation and give rise to complications like a) ameloblastoma, b) squamous cell carcinoma and c) mucoepidermoid carcinoma.
Eruption cyst also called eruption hematoma is the soft tissue variant of dentigerous cyst.
📖REFERENCES AND FURTHER READING
Shear M, Speight PM. Cysts of the Oral and Maxillofacial Regions. 4 th ed. Blackwell Munksgaard; 2007.
Neville BW, Damm DD, Allen CM, Chi A. Oral and Maxillofacial Pathology. South Asian ed. Elsevier; 2016.
Rajendran R, Sivapathasundaram B. Shafer’s Textbook of Oral Pathology. 7th ed. Elsevier; 2012.
Regezzi JA, Sciubba JJ, Jordan RCK. Oral Pathology: Clinical Pathologic Correlations. 5 th ed. Elsevier; 2007.
Sapp JP, Eversole LR, Wysocki GP. Contemporary Oral and Maxillofacial Pathology. 2 nd ed. Mosby; 2004.
Wood NK, Goaz PW. Differential Diagnosis of Oral and Maxillofacial Lesions. 5 th ed. Mosby; 1997.