
Fibrous Dysplasia (Notes & Video)

Fibrous dysplasia (FD) is a developmental fibro-osseous lesion characterized by substitution of normal bone by proliferating fibrous tissue and irregular woven (immature) bone.
FD can be of different types depending on the number of bones involved:
Monostotic FD --> single bone affected
Polyostotic FD --> multiple bones affected
Craniofacial FD --> multiple bones limited to the craniofacial complex
FD, apart from having bone lesions can also be associated with skin and endocrine abnormalities.
✋Just before you proceed
The video in this post talks about the clinical and radiology features of fibrous dysplasia. However the notes cover the entire topic.
Here’s the video 👉 that talks about the pathogenesis and histopathology of fibrous dysplasia.
💡Know Thy Facts!
The term “dysplasia” in fibrous dysplasia, refers to the abnormal/ disordered production and development of bone. It does not refer to or signify the presence of “atypia” or “pre-malignant” features that are described in potentially malignant mucosal lesions like leukoplakia! ETIOLOGY & PATHOGENESIS
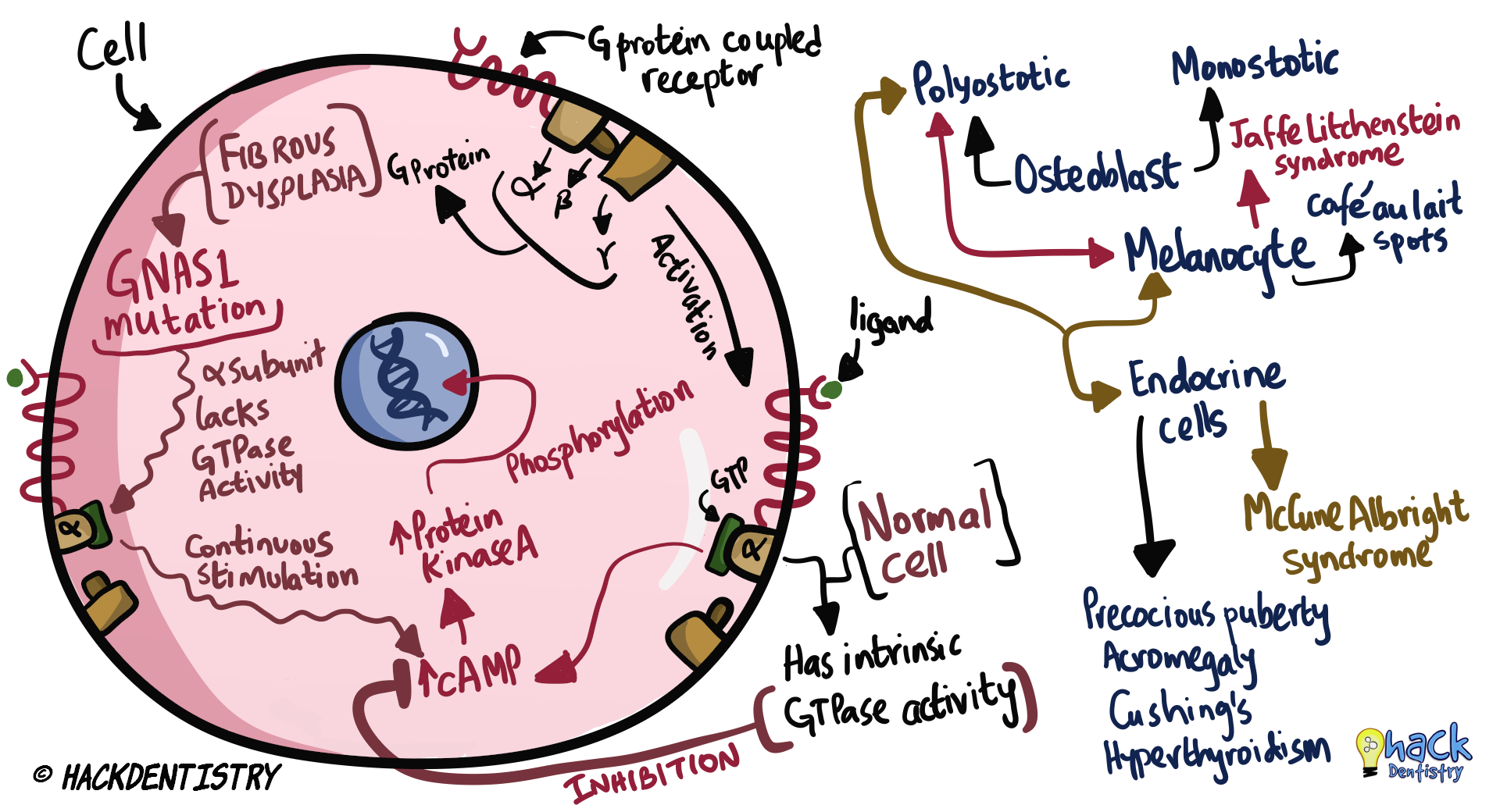
FD is caused due to a mutation in the GNAS1 (Guanine nucleotide-binding protein, alpha stimulating activity polypeptide) gene.
GNAS1 gene encodes for the α-subunit of G protein.
NORMALLY
G protein stimulates (via α-subunit) --> production of cAMP --> cAMP activates protein kinase A --> phosphorylation of target genes leading to increased proliferation of cells (osteoblastic, melanocytic or endocrine).
GTPase activity (intrinsic to α-subunit of G-protein) stops the production of cAMP --> proliferation of cells in control.
IN FIBROUS DYSPLASIA
Mutation of GNAS1 gene --> abnormal α-subunit of G protein --> has no intrinsic GTPase activity.
Hence there is uncontrolled production of cAMP --> leading to uncontrolled and abnormal proliferation of cells (osteoblastic, melanocytic or endocrine).
INCREASED cAMP IN FIBROUS DYSPLASIA
Abnormal differentiation and hyper-proliferation of immature osteoblasts --> leads to bone manifestations (monostotic, polyostotic, craniofacial).
Melanocyte abnormalities --> abnormal pigmentation of skin - café au lait spots/pigmentation.
Hyperplasia and excessive function of different endocrine cell types --> endocrinopathies – precocious puberty, acromegaly, Cushing syndrome, hyperthyroidism.
CLINICAL FEATURES
MONOSTOTIC FIBROUS DYSPLASIA
FD is considered monostotic when only one bone is involved.
Most common type of FD --> 70-80% FD cases are monostotic.
Bones usually affected --> jaws, other craniofacial bones, femur
Usually affects individuals in the 2nd to 3rd decade.
Does not have any gender predilection.
Monostotic FD usually affects the maxilla more often than the mandible.
💡Know Thy Facts!
FD is truly monostotic when only the mandible is involved. However, when the maxilla is affected, other adjacent bones in the craniofacial complex may also be involved like the zygoma, sphenoid, ethmoid, frontal and temporal bones. Hence most often, monostotic FD involving the maxilla would end up involving other adjacent bones and is better termed Craniofacial FD!
Individuals with FD in the craniofacial complex have been described to have “leonine facies” (facial features resembling a lion) also called “leontiasis ossea”.POLYOSTOTIC FIBROUS DYSPLASIA
FD is considered polyostotic when two or more bones are involved.
20-30% FD cases are polyostotic.
Bones usually affected --> craniofacial bones, pelvis, spine, shoulder girdle.
Usually affects children below 10 years.
Polyostotic FD has a female predilection.
When jaw bones are involved, maxilla is more often involved than the mandible.
Polyostotic FD is most often involved with other syndromes:
McCune Albright syndrome --> polyostotic FD + skin pigmentations (café au lait spots) + endocrine abnormalities
Jaffe Litchenstein syndrome --> polyostotic FD + skin pigmentations (café au lait spots)
Mazabraud syndrome --> FD and intramuscular myxomasSKIN PIGMENTATIONS
Café au lait spots are hyperpigmented macules affecting the skin.
These macules have irregular margins --> described as resembling the “Coast of Maine”.
This is in contrast to the café au lait spots seen in neurofibromatosis where the margins of the macules are regular and smooth --> described as resembling the “Coast of California”.
ENDOCRINE ABNORMALITIES
Precocious puberty
Acromegaly
Cushing’s syndrome
Hyperthyroidism
Hyperparathyroidism
CRANIO-FACIAL/ORAL/DENTAL MANIFESTATIONS
Unilateral, painless swelling of jaws – usually maxilla.
Asymmetry of face --> bulging of canine fossa/zygoma.
Displacement of teeth and malocclusion.
Disturbed tooth eruption.
When mandible is involved, there may be a bucco-lingual expansion along with an expansion/bulging of the inferior border.
When other bones (other than the maxilla) of the craniofacial complex are involved, there may also be --> vision changes, hearing loss, airway obstruction.
COMPLICATIONS
0.4-1% chances of malignant transformation to osteosarcoma, fibrosarcoma and rarely chondrosarcoma.
RADIOLOGY FEATURES
The lesion is not well defined and circumscribed; is diffuse blending with the normal bone.
Classical appearance of FD --> diffuse and “frosty” radiopacity --> described as a “ground glass” appearance.
Also described as having a peau d’orange (orange peel) appearance.
Other radiology manifestations --> unilocular/multilocular radiolucencies, mixed radiolucent-radiopaque, fingerprint pattern.
💡Know Thy Facts!
Malformation of proximal femur in polyostotic FD --> “sheperd’s crook” or “hockey stick” deformity!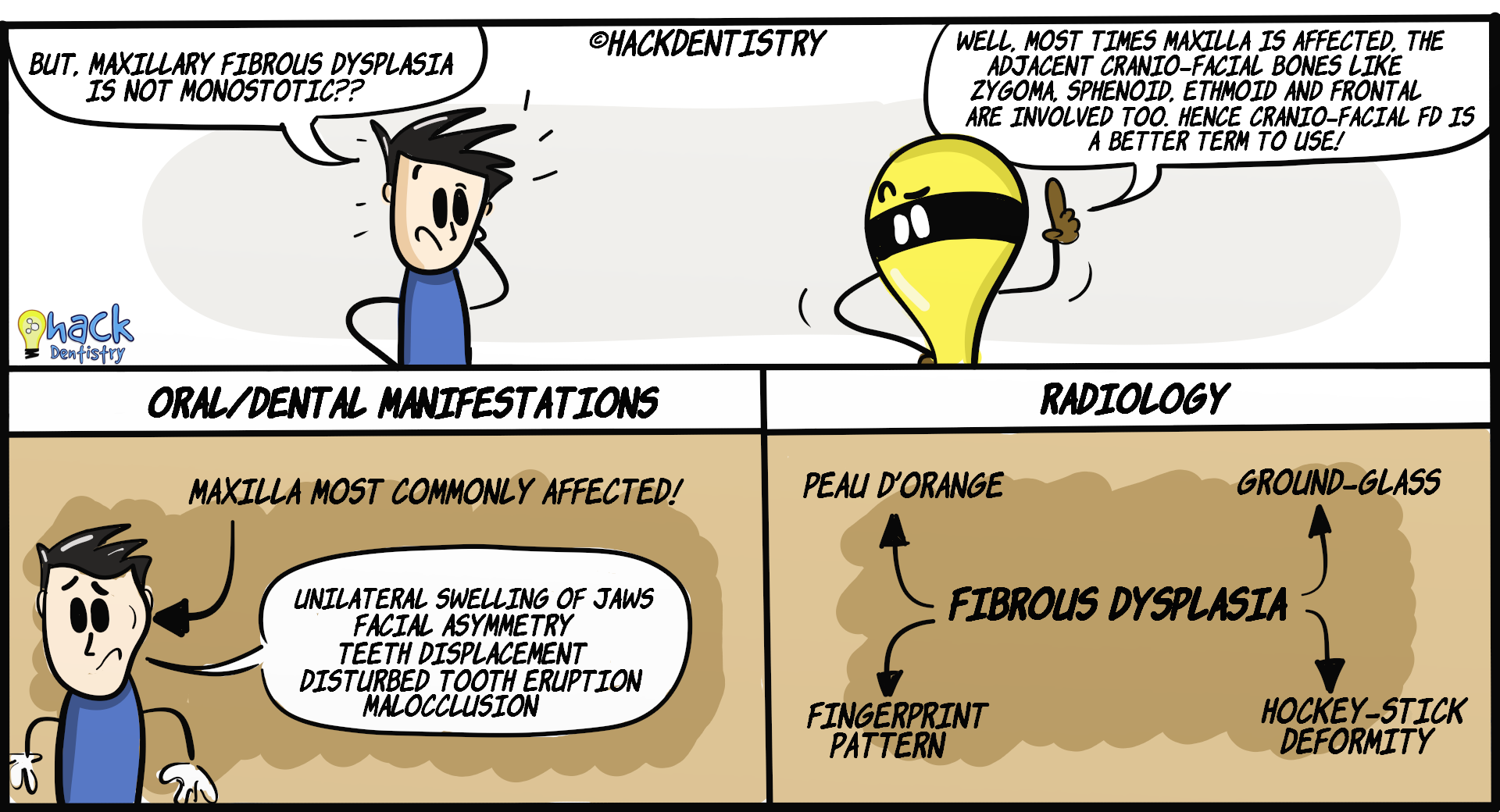
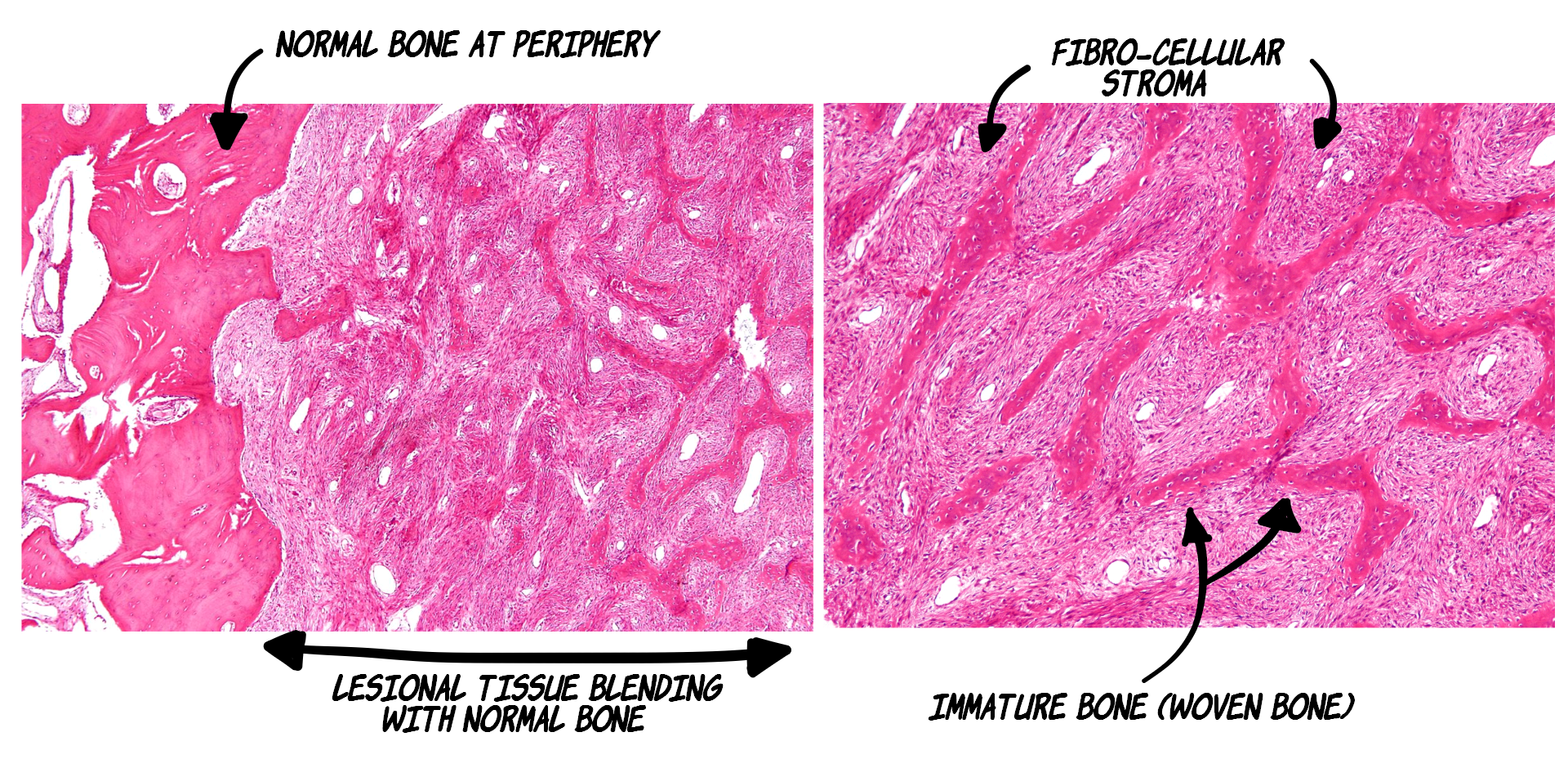
HISTOPATHOLOGY FEATURES
Presence of numerous immature/woven bone trabeculae in a mild to moderately cellular, fibrous connective tissue.
Bone trabeculae have irregular curves --> described to have a resemblance to chinese letter/characters.
Lesional bone fuses with normal bone at the periphery.
Osteoblastic rimming (trabeculae surrounded by osteoblasts) absent.
Peritrabecular clefting (artefact --> retraction of stroma from bone) is a characteristic feature of FD.
TREATMENT
FD usually stops progressing after puberty.
Surgical reduction/contouring may be needed for esthetic and functional purposes.
Orthodontic corrections and other surgical procedures to correct malocclusion.
There may be a possibility of a recurrence in rare cases.
✅HIGHLIGHTS - VIVA & ENTRANCE EXAM PERSPECTIVE
a) Monostotic FD --> single bone affected, b) Polyostotic FD --> multiple bones affected, c) Craniofacial FD --> multiple bones limited to the craniofacial complex.
FD is caused due to a mutation in the GNAS1 (Guanine nucleotide-binding protein, alpha stimulating activity polypeptide) gene.
Most common type of FD --> 70-80% FD cases are monostotic.
Monostotic FD usually affects the maxilla more often than the mandible.
Most often, monostotic FD involving the maxilla would end up involving other adjacent bones and is better termed Craniofacial FD!
Individuals with FD in the craniofacial complex have been described to have “leonine facies” (facial features resembling a lion) also called “leontiasis ossea”.
McCune Albright syndrome --> polyostotic FD + skin pigmentations (café au lait spots) + endocrine abnormalities.
Jaffe Litchenstein syndrome --> polyostotic FD + skin pigmentations (café au lait spots).
Mazabraud syndrome --> FD and intramuscular myxomas.
These macules have irregular margins --> described as resembling the “Coast of Maine”.
Classical appearance of FD --> diffuse and “frosty” radiopacity described as a “ground glass” appearance.
Also described as having a peau d’orange (orange peel) appearance.
Malformation of proximal femur in polyostotic FD --> “sheperd’s crook” or “hockey stick” deformity!
Presence of numerous immature/woven bone trabeculae in a mild to moderately cellular, fibrous connective tissue.
Peritrabecular clefting (artefact --> retraction of stroma from bone) is a characteristic feature of FD.
0.4-1% chances of malignant transformation to osteosarcoma, fibrosarcoma and rarely chondrosarcoma.
📖REFERENCES AND FURTHER READING
Pereira TDSF, Gomes CC, Brennan PA, Fonseca FP, Gomez RS. Fibrous dysplasia of the jaws: Integrating molecular pathogenesis with clinical, radiological, and histopathological features. J Oral Pathol Med. 2019; 48(1):3-9.
Marie PJ. Cellular and molecular basis of fibrous dysplasia.Histol Histopathol. 2001 Jul;16(3):981-8.
Brannon RB, Fowler CB. Benign fibro-osseous lesions: a review of current concepts. Adv Anat Pathol. 2001;8(3):126-43.
Eversole R, Su L, ElMofty S. Benign Fibro-Osseous Lesions of the Craniofacial Complex A Review. Head Neck Pathol. 2008; 2(3): 177–202.
Neville BW, Damm DD, Allen CM, Chi A. Oral and Maxillofacial Pathology. South Asian ed. Elsevier; 2016.
Regezzi JA, Sciubba JJ, Jordan RCK. Oral Pathology: Clinical Pathologic Correlations. 5 th ed. Elsevier; 2007.
Rajendran R, Sivapathasundaram B. Shafer’s Textbook of Oral Pathology. 7th ed. Elsevier; 2012.
🔖Histopathology Picture attribution:
Nephron: https://commons.wikimedia.org/wiki/File:Fibrous_dysplasia_-_low_mag.jpg
Nephron: https://commons.wikimedia.org/wiki/File:Fibrous_dysplasia_-_intermed_mag.jpg
Both pictures licensed under Creative Commons Attribution-Share Alike 3.0 Unported license/modified
{kind=link}
{kind=link}