
Gingiva (Note)

Gingiva is that portion of the oral mucosa that attaches to the alveolar process of the jaw and surrounds the cervical portions of the teeth.
💡 Macroscopically, the gingiva is divided into the following:
- Marginal or free gingiva
- Attached gingiva
- Interdental gingivaApical to the attached gingiva, is the alveolar mucosa surrounding the lower part of the alveolar bone.
Microscopically the gingiva is a keratinized epithelium, predominantly parakeratinized (75%).
MACROSCOPY/GENERAL ANATOMY OF GINGIVA
Marginal or free gingiva:
The marginal or free gingiva is a portion of movable gingiva surrounding the tooth in a collar like fashion.
This portion of the gingiva is called “free gingiva” as it is unattached to the periosteum of the underlying bone.
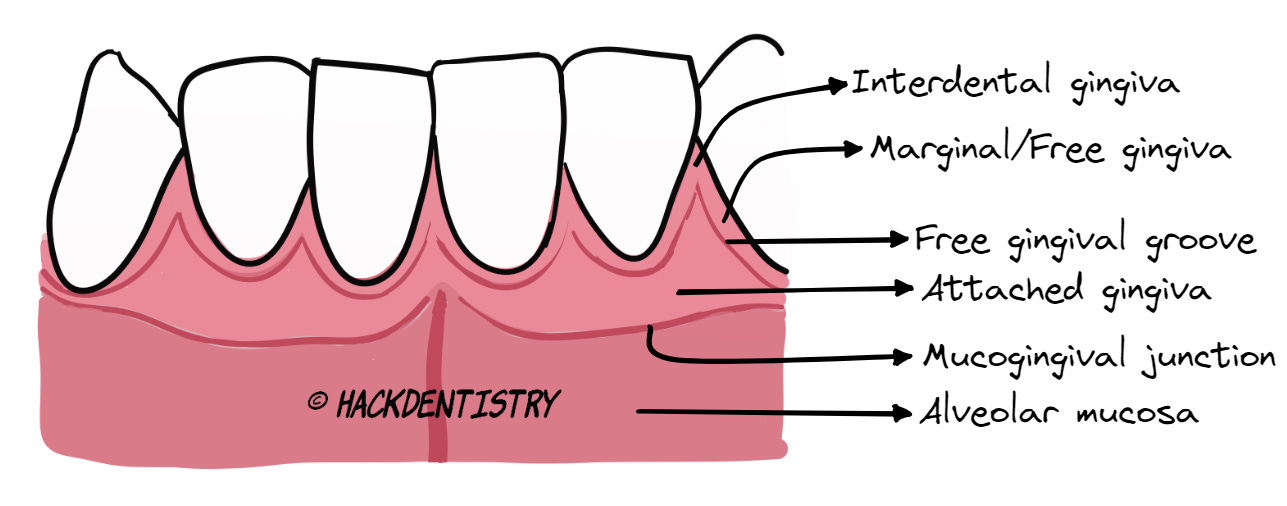
The marginal gingiva (MG) is continuous with the attached gingiva apically and is separated (from the attached gingiva) by a shallow groove called the free gingival groove (FGG).
The MG, hence, is that part of the movable gingiva that is seen between the gingival margin coronally and the FGG apically.
The FGG may be approximately at the level of the cemento-enamel junction (CEJ) and is apparent in only 30-40% of individuals.
The inner surface of the MG forms the wall of the gingival sulcus.
What and where is the Gingival Sulcus?
- The crevice or gap seen between the MG and the tooth surface is called the gingival sulcus.
- The inner portion of the free or marginal gingiva forms the wall of the gingival sulcus on one side and the sulcus is bound by the tooth surface on the other.
- The inner portion of the free gingiva forming the wall of the sulcus is lined by the sulcular epithelium. The sulcular epithelium is non-keratinized.
- The sulcular epithelium is apically continuous with the junctional epithelium.
- The junctional epithelium, like the sulcular epithelium is non-keratinized.
- The sulcular depth in healthy gums (taking into consideration a mild level of chronic inflammation) ranges from 2-3 mm (Carranza) and this depth could increase with age or disease. A depth of more than 3 mm suggests periodontal disease.
Note: Sulcular depth could range from 0.5-3mm (Berkovitz and Tencate) and a probing depth greater than 3 mm indicates periodontal disease.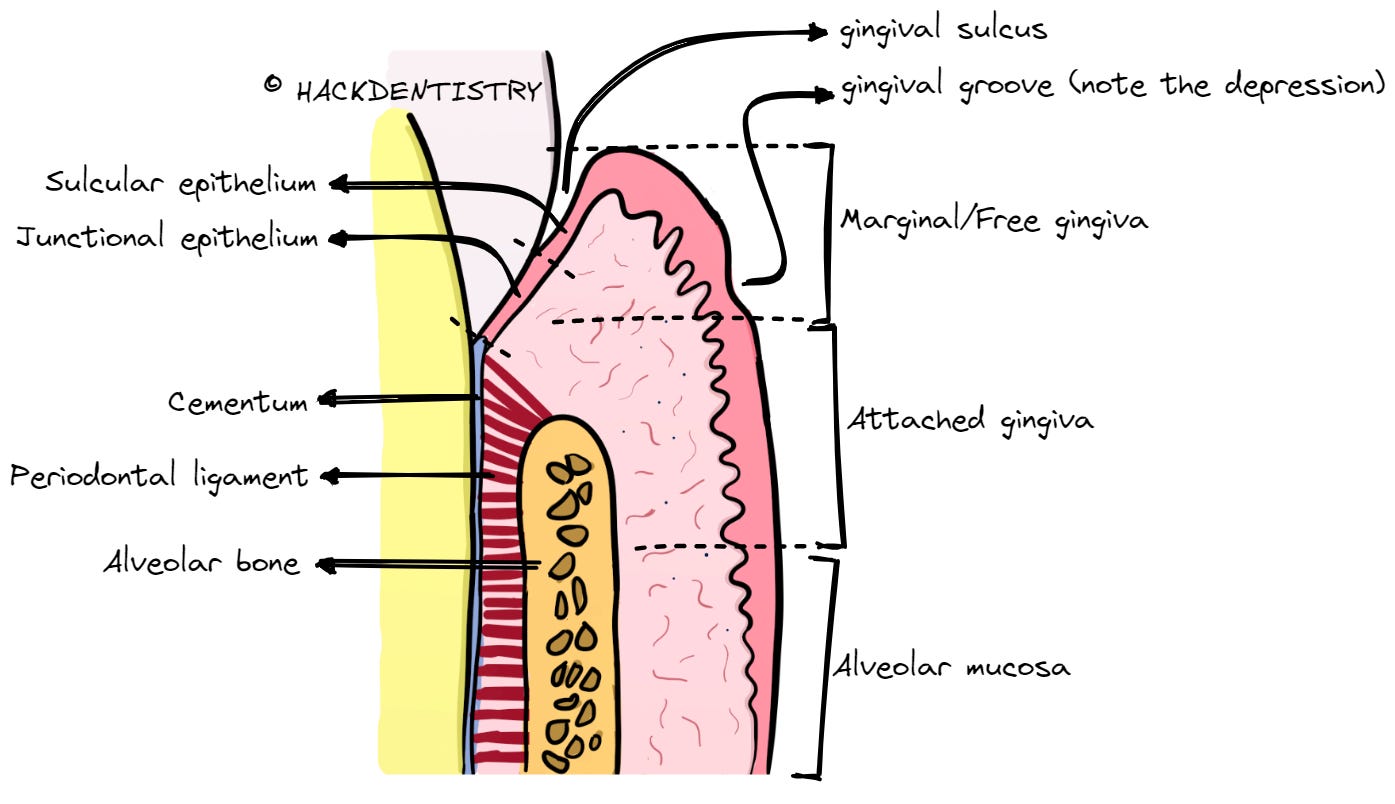
Attached gingiva:
It is that part of the gingiva that is firmly attached to the underlying periosteum of the alveolar bone and cementum of the tooth.
The attached gingiva is coronally continuous with the marginal gingiva (MG) and is apically continuous with the alveolar mucosa.
Coronally, attached gingiva is demarcated from the MG by a free gingival groove and is apically demarcated from the alveolar mucosa by the mucogingival junction.
The width of the attached gingiva is usually more in the maxilla than in the mandible.
The surface of healthy attached gingiva show small depressions. This appearance is called “stippling”.
The epithelium of the attached gingiva is keratinized.
NOTE
- The attached gingiva lacks a submucosa and the lamina propria is tightly bound to the underlying periosteum of alveolar bone.
- Muco-gingival junction is absent on the palatal surface of the maxilla.
What is stippling?
The surface texture of the attached gingiva and the center of the interdental gingiva show alternate protuberances and depressions. This texture resembles an orange peel and is called "stippling". Stippling is due to the connective tissue papillae projecting into the epithelium. Inflamed gingiva shows loss of stippling and has a rather smooth surface texture.Interdental gingiva:
Interdental gingiva is that part of the gingiva between two adjacent teeth.
It conforms to the shape of the interdental space.
It is usually wedge or triangular shaped when seen buccally or lingually.
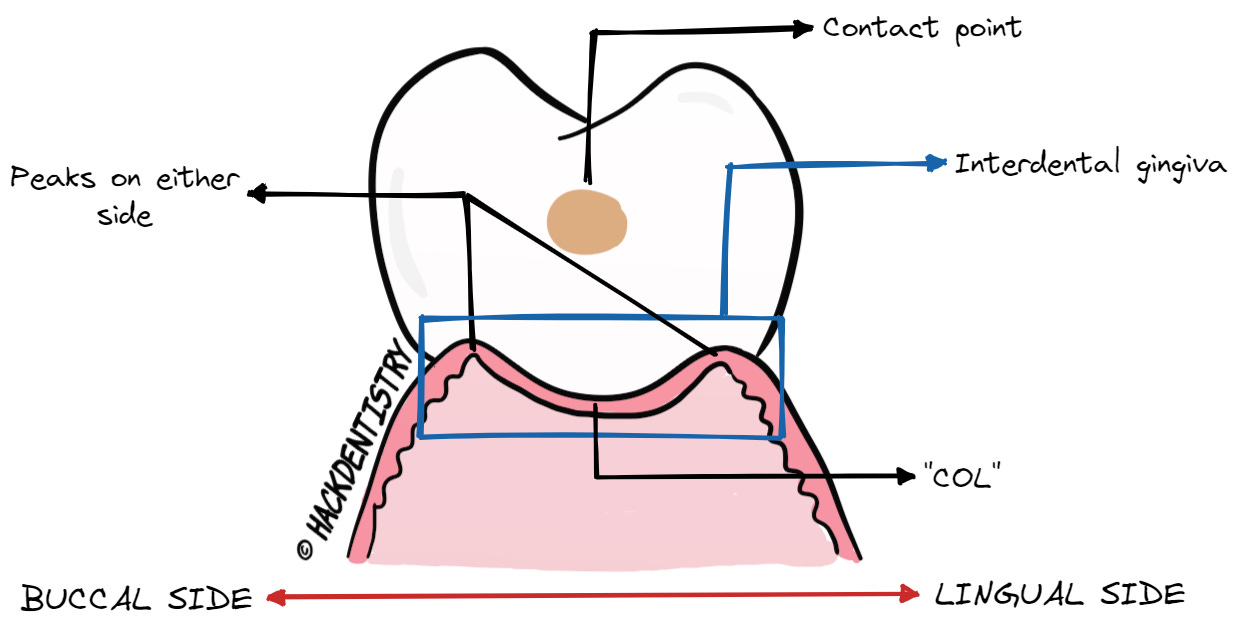
However, in the bucco-lingual plane of the posterior teeth, the interdental gingiva may have two peaks, one each on the buccal and lingual side and a curved depression (of gingiva) between the two peaks.
The curved depression of gingival tissue seen in the bucco-lingual plane runs just below the contact points of the two adjacent teeth. This portion of the interdental gingiva is called “Col”.
Col is non-keratinized.
The interdental gingiva is absent when the two adjacent teeth are spaced.
MICROSCOPY (IN BRIEF)
- The gingival epithelium is keratinized epithelium. The epithelium is predominantly parakeratinized.
- The marginal, attached and interdental gingiva are keratinized.
- The sulcular epithelium, junctional epithelium and “col” are non-keratinized.HIGHLIGHTS - VIVA & ENTRANCE EXAM PERSPECTIVE
Macroscopically, the gingiva is divided into the following -> a) Marginal or free gingiva, b) Attached gingiva and c) Interdental gingiva.
Microscopically the gingiva is a keratinized epithelium, predominantly parakeratinized (75%).
The marginal or free gingiva is a portion of movable (unattached) gingiva surrounding the tooth in a collar like fashion.
The marginal gingiva (MG) is continuous with the attached gingiva apically and is separated (from the attached gingiva) by a shallow groove called the free gingival groove (FGG).
The crevice or the small space between the tooth and the marginal gingiva forms the gingival sulcus.
The inner portion of the free gingiva forming the wall of the sulcus is lined by the sulcular epithelium. The sulcular epithelium is non-keratinized.
The junctional epithelium, like the sulcular epithelium is non-keratinized.
The attached gingiva is coronally continuous with the marginal gingiva (MG) and is apically continuous with the alveolar mucosa.
Coronally, attached gingiva is demarcated from the MG by a free gingival groove and is apically demarcated from the alveolar mucosa by the mucogingival junction.
The surface of healthy attached gingiva show small depressions. This appearance is called “stippling”.
Interdental gingiva is usually wedge or triangular shaped when seen buccally or lingually.
The curved depression of gingival tissue seen in the bucco-lingual plane runs just below the contact points of the two adjacent teeth. This portion of the interdental gingiva is called “Col”.
Col is non-keratinized.
REFERENCES AND FURTHER READING
Newman MG, Takei H, Klokkevold PR, Carranza FA. Carranza’s Clinical Periodontology. 10 th ed. Elsevier; 2009.
Lindhe J, Lang NK, Karring T. Clinical periodontology and implant dentistry. 5th ed. Blackwell Munksgaard;2008.
Shalu Bathla. Textbook of Periodontics. 2nd ed. Jaypee Brothers Medical Publishers; 2021.
Berkovitz BKB, Hollan GR, Moxham BJ. Oral Anatomy, Histology and Embryology. 4th ed. Mosby Elsevier; 2009.
Nanci A. Tencate’s Oral Histology. Development, Structure and Function. 8th ed. Elsevier; 2013.
Kumar GS. Orban’s Oral Histology and Embryology.13th ed. Elsevier; 2011.