
Leukoplakia (Notes & Video)

Trivia
This was the first ever video I created for HackDentistry and was released in December 2016.
“Leuko” stands for white and “plakia” for patch. Leukoplakia is a white patch occurring in the oral mucosa, which cannot be diagnosed as any other definable lesion.
Leukoplakia is defined as --> “a white plaque of questionable risk having excluded (other) known diseases or disorders that carry no increased risk for cancer”.
💡Know Thy Facts!
Leukoplakia is a diagnosis of exclusion. There are a number of “leukoplakia-like” white lesions that manifest in the oral cavity (refer topic on “White lesions-Differential diagnosis”). For example, oral lichen planus (OLP) may manifest as a plaque lesion resembling leukoplakia. However, OLP has definitive clinical (white striae elsewhere in the oral cavity) and histopathology features. A clinician should rule out such definitive white lesions, before a clinical diagnosis of “leukoplakia” can be made.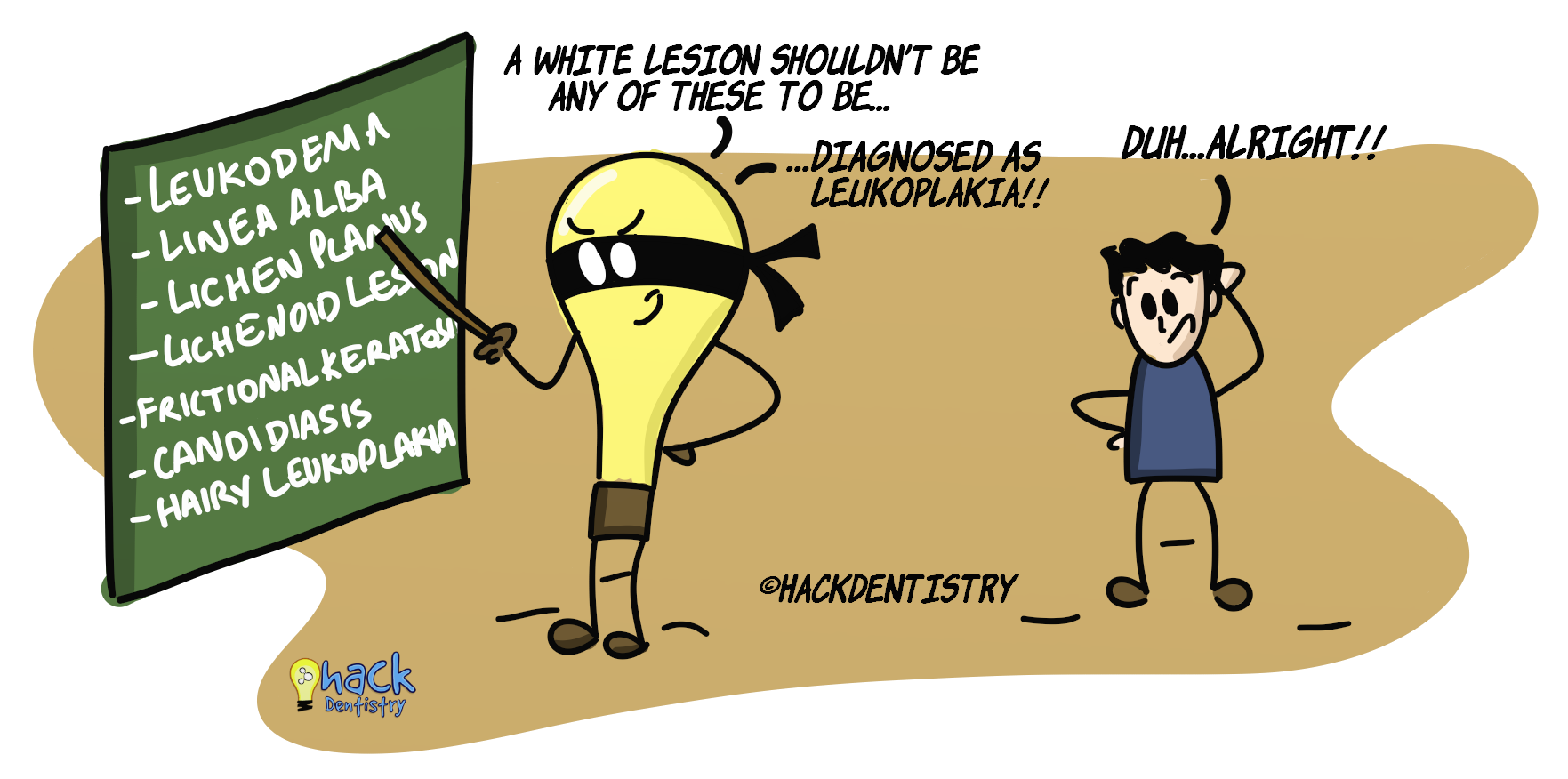
ETIOLOGY
Leukoplakia is predominantly induced by tobacco --> smoked (cigar, cigarette, pipe, beedi) and smokeless (chewing tobacco, dry/wet snuff).
Alcohol is known to be synergistic with tobacco in causing leukoplakia.
Candida albicans is known to cause a lesion called candidal leukoplakia otherwise called chronic hyperplastic candidiasis. However, it is not clear whether candida causes the lesion or candida is superimposed on an existing leukoplakia.
Leukoplakia without a known etiology is called idiopathic leukoplakia.
💡Know Thy Facts!
Snuff/finely powdered tobacco most times induces a lesion called “Tobacco pouch keratosis”. This is white keratotic and wrinkled lesion that resembles leukoplakia. It is important to distinguish this lesion from leukoplakia, as it usually disappears on cessation of the habit and also does not show dysplasia histopathologically. Long term usage of snuff could induce leukoplakia.CLINICAL FEATURES
Leukoplakia is the most common potentially malignant disorder and has a worldwide prevalence of 2%.
Manifests in the elderly --> people >40 years of age; mostly in males.
Common oral sites - Asian population --> buccal mucosa, mandibular vestibule and gingiva; Western population --> lateral margin of tongue, floor of mouth.
Leukoplakia occurring in the floor of the mouth or tongue have increased chances of dysplasia and malignant transformation.
Two clinical types of leukoplakia --> homogenous and non-homogenous.
Homogenous types are known to have a better prognosis than non-homogenous types.
HOMOGENOUS LEUKOPLAKIA
Is a predominantly white lesion (patch).
The surface of the lesion may be flat, wrinkled, corrugated or may have cracks (note that the surface is not irregular --> uniform texture).
NON-HOMOGENOUS LEUKOPLAKIA
It could be a predominantly white or a white & red lesion.
The surface of the lesion is irregular --> nodular, exophytic or verrucous.
💡Know Thy Facts!
When defining a clinical type of leukoplakia, the adjective “homogenous” refers to both, the predominantly white colour of the lesion and an almost uniformly flat surface (texture). [Homogenous --> white colour & regular texture].
Leukoplakias with either a non-uniform colour or irregular texture are called “non-homogenous”. For example, it could be predominantly white but may be nodular, exophytic or verrucous (irregular texture). Or, the lesion could be flat and almost uniform in texture but may be a white & red lesion (non-uniform colour). [Non-homogenous --> white colour & irregular texture/ non-uniform colour & regular texture/non-uniform colour & irregular texture].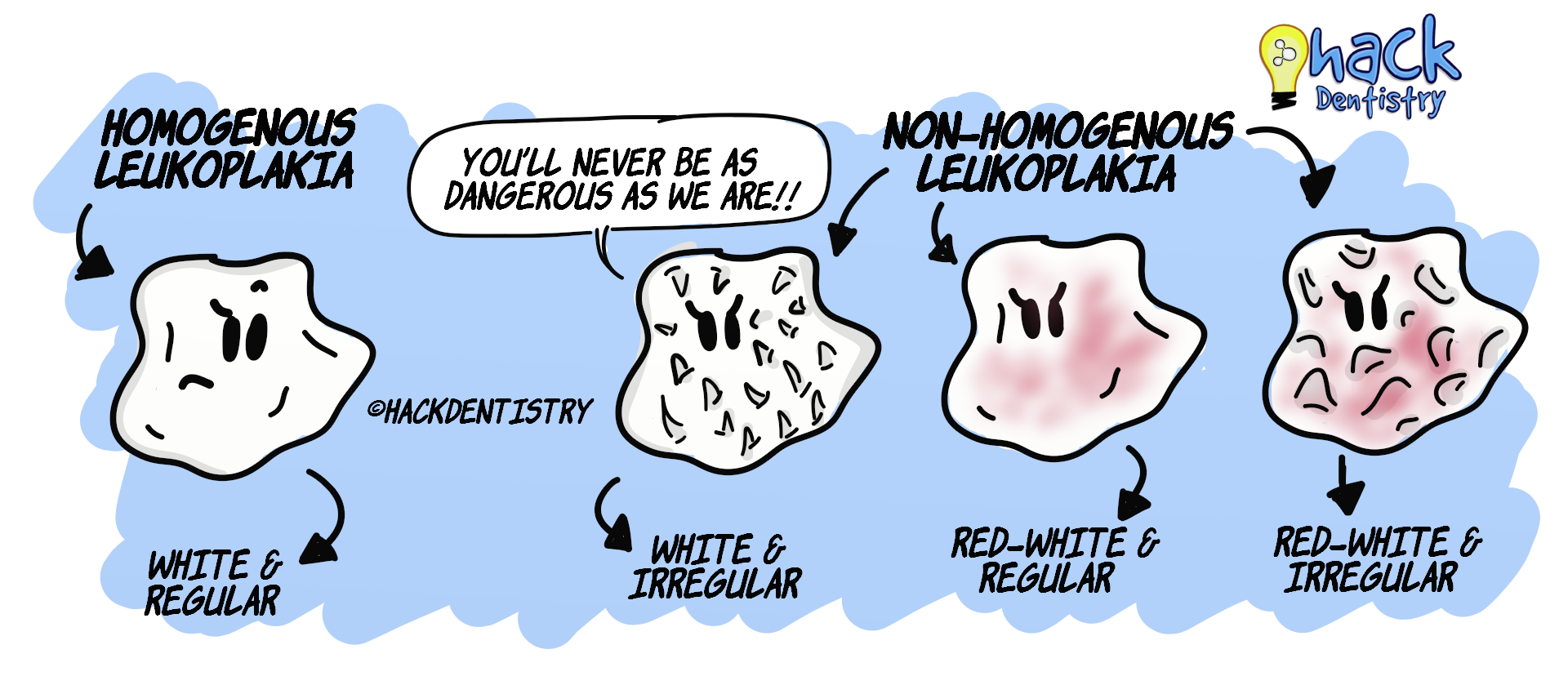
Nodular leukoplakia --> Leukoplakia with nodular or granular surface irregularities.
Verrucous leukoplakia -> Leukoplakia with an exophytic, verrucous or wart like projections.
Speckled leukoplakia/erythroleukoplakia --> Leukoplakia with red patches manifesting as a white & red lesion. This variety of leukoplakia is to be dealt with caution as it usually shows dysplasia or even carcinoma histopathologically.
Leukoplakia has a malignant transformation rate ranging from 1-17.5%.

Leukoplakia has an increased risk of malignant transformation when it:
Occurs in women
Is present for a long duration
Appears in non-smokers
Is located on the ventral tongue and floor of mouth
Has an extensive size
Manifests dysplasia
💡A NOTE ON PROLIFERATIVE VERRUCOUS LEUKOPLAKIA
- Proliferative verrucous leukoplakia(PVL) is a rare high risk form of leukoplakia.
- It starts off as a homogenous leukoplakia, that over time, spreads to become diffuse and multi-focal (involves many sites).
- PVL is persistent, irreversible and resistant to all forms of treatment with a high recurrence rate.
- It has a malignant transformation rate of 70-100%.HISTOPATHOLOGY FEATURES
A biopsy of leukoplakia lesion may reveal a range of findings.
Findings could range from --> hyperkeratosis and hyperplasia --> dysplasia (mild/moderate/severe) --> carcinoma-in situ --> squamous cell carcinoma (refer topic on “Epithelial dysplasia”).
TREATMENT
In the absence of dysplasia, surgical excision may not be necessary. Other treatment modalities may be considered --> Vitamin A, C and E, beta carotene and diet high in anti-oxidants are recommended. Although, some recommend surgical excision regardless of the presence or absence of dysplasia.
Some regard leukoplakias on suspicious sites like ventral tongue and floor of mouth to be excised regardless of dysplasia status (present or absent).
Moderate to severe dysplasia status would mandate a surgical excision.
✅HIGHLIGHTS - VIVA & ENTRANCE EXAM PERSPECTIVE
Leukoplakia is “a white plaque of questionable risk having excluded (other) known diseases or disorders that carry no increased risk for cancer”.
Snuff/finely powdered tobacco most times induces a lesion called “Tobacco pouch keratosis”.
Leukoplakia without a known etiology is called idiopathic leukoplakia.
Leukoplakia is the most common potentially malignant disorder.
Leukoplakia occuring in the floor of the mouth or tongue have increased chances of dysplasia and malignant transformation.
Homogenous leukoplakia --> white colour & regular (surface) texture.
Non-homogenous leukoplakia --> white colour & irregular (surface) texture/ non-uniform colour & regular (surface) texture/ non-uniform colour & irregular (surface) texture.
Speckled leukoplakia is to be dealt with caution as it usually shows dysplasia or even carcinoma histopathologically.
Proliferative verrucous leukoplakia (high risk variant of leukoplakia) starts off as a homogenous lesion, that over time, spreads to become diffuse and multi-focal (involves many sites).
📖REFERENCES AND FURTHER READING
van der Waal I, Schepman KP, van der Meij EH, Smeele LE. Oral leukoplakia: a clinicopathological review. Oral Oncol. 1997 Sep;33(5):291-301.
Carrard VC, van der Waal I. A clinical diagnosis of oral leukoplakia; A guide for dentists. Med Oral Patol Oral Cir Bucal. 2017;23(1):e59–e64.
Dionne KR, Warnakulasuriya S, Zain RB, Cheong SC. Potentially malignant disorders of the oral cavity: current practice and future directions in the clinic and laboratory. Int J Cancer. 2015 Feb 1;136(3):503-15.
Warnakulasuriya S. Clinical features and presentation of oral potentially malignant disorders. Oral Surg Oral Med Oral Pathol Oral Radiol. 2018 Jun;125(6):582-590.
Neville BW, Damm DD, Allen CM, Chi A. Oral and Maxillofacial Pathology. South Asian ed. Elsevier; 2016.
Rajendran R, Sivapathasundaram B. Shafer’s Textbook of Oral Pathology. 7th ed. Elsevier; 2012.
Regezzi JA, Sciubba JJ, Jordan RCK. Oral Pathology: Clinical Pathologic Correlations. 5 th ed. Elsevier; 2007.
Sapp JP, Eversole LR, Wysocki GP. Contemporary Oral and Maxillofacial Pathology. 2 nd ed. Mosby; 2004.
Wood NK, Goaz PW. Differential Diagnosis of Oral and Maxillofacial Lesions. 5 th ed. Mosby; 1997.