
Odontogenic keratocyst (Note & Video)

Odontogenic keratocyst (OKC) is the second most common developmental odontogenic cyst after dentigerous cyst. It makes up around 10% of all odontogenic cysts occurring in the oral cavity.
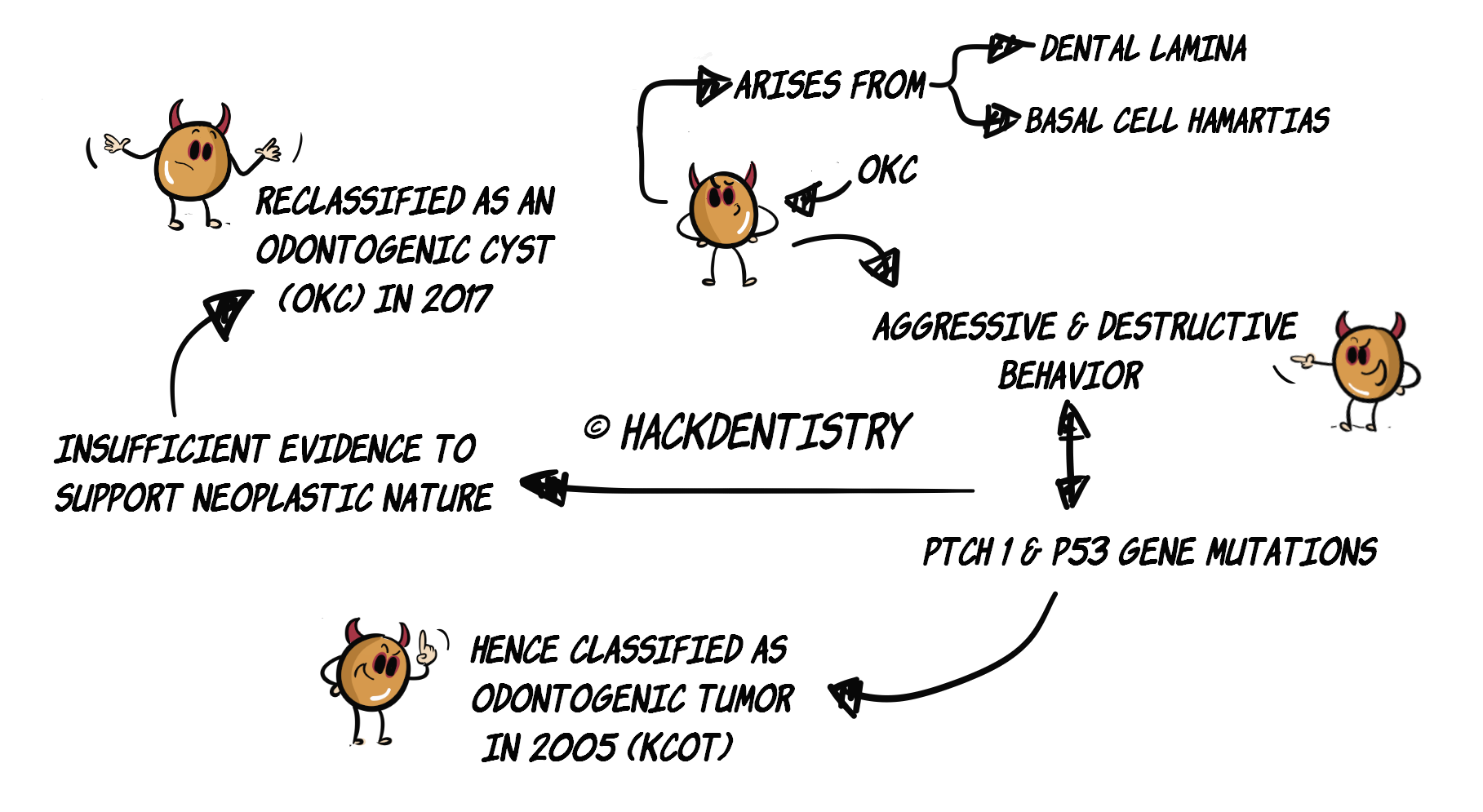
This cyst is believed to develop from --> a) from the rests of the dental lamina and b) extensions of the basal cells from the overlying epithelium (“basal cell hamartias” or “basal cell offshoots”).
It is called odontogenic keratocyst because it is “odontogenic” in origin and the cyst lumen is filled with “keratin”.
OKC has an aggressive and destructive behavior as compared to other odontogenic cysts. Also, some OKCs have been reported to have genetic mutations in the PTCH1 and P53 genes giving it a greater growth potential.
Hence, many pathologists considered OKC to be neoplastic. The 2005 World Health Organization (WHO) monograph on Head and Neck tumors classified it as an odontogenic tumor and named it “Keratocystic odontogenic tumor (KCOT)” in 2005.
💡RECENT UPDATES
The WHO consensus group in 2017, have however reinstated the name Odontogenic keratocyst and have reclassified the lesion as an odontogenic cyst. The group felt there was insufficient evidence to support its neoplastic nature.
CLINICAL FEATURES
OKC predominantly occurs in the second and third decades of life.
Has a slight male predilection.
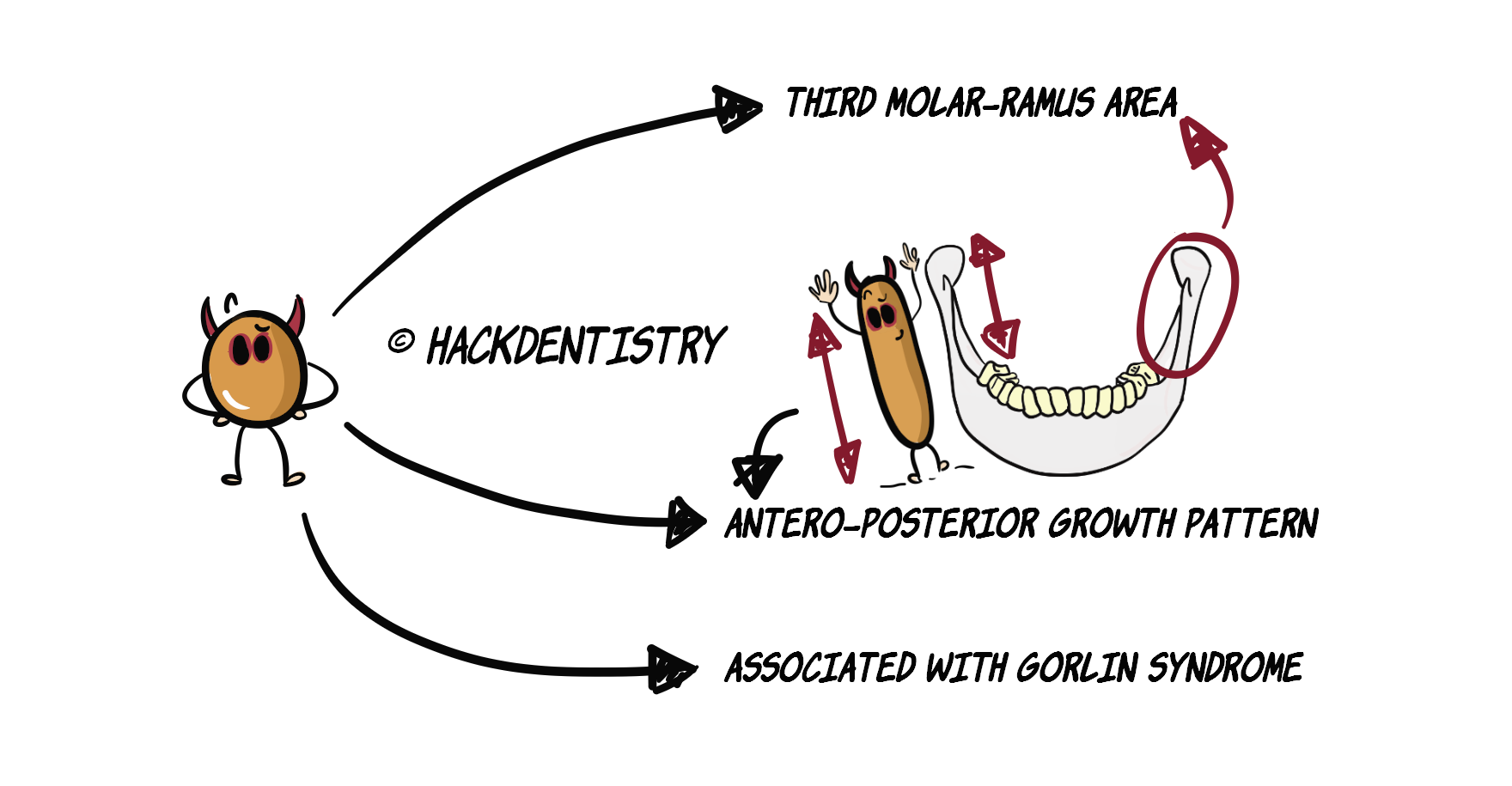
Predominantly occurs in the mandible usually in the third molar-ramus area.
OKCs may range from being small and asymptomatic, to large lesions causing swelling and pain.
A characteristic feature of OKC is its antero-posterior growth within the marrow cavity of the bone, causing no bone expansion despite its size.
OKC has been reported to be associated with nevoid basal cell carcinoma syndrome or Gorlin syndrome. At least 90% of patients with this syndrome have been reported to have multiple OKCs.
RADIOLOGY FEATURES
OKC does not have a characteristic radiographic appearance. It may mostly show a unilocular radiolucency though large lesions may appear mutlilocular.
Around 25-40% of OKCs are associated with an unerupted tooth, showing a pericoronal radiolucency mimicking a dentigerous cyst.
Large lesions may show buccal cortical expansion.
HISTOPATHOLOGY FEATURES
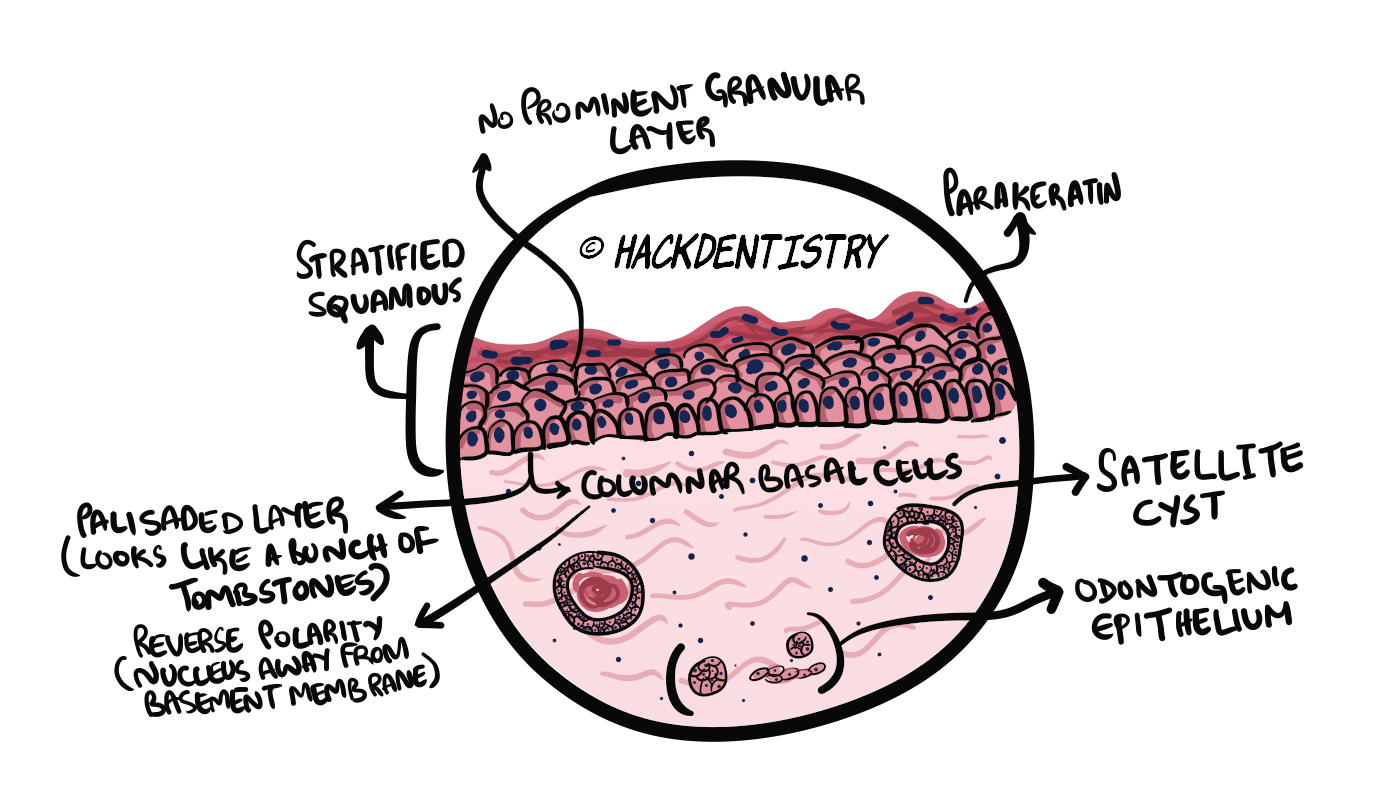
The epithelial lining is composed of:
stratified squamous epithelium usually 6-10 cells in thickness.
corrugated or wavy parakeratinized layer
cuboidal to columnar basal cell layer, that is palisaded, described as having a picket fence or tomb stone appearance.
The epithelium does not have a prominent granular layer as present in orthokeratinized odontogenic cyst (OOC) (a factor differentiating OKC from OOC).
The fibrous wall/connective tissue may harbour satellite cysts, cords or islands of odontogenic epithelium.
The epithelium- connective tissue interface is flat and has no rete ridges.
The lumen may contain a straw colored clear fluid or a cheesy material that represents keratin under the microscope.
💡OKC HAS A HIGH RECURRENCE RATE!
- Incomplete removal of OKC may lead to development of new cysts due to the retained satellite cysts and odontogenic islands or rests in the cyst wall.
- The epithelial lining is thin and friable, and may be difficult to completely remove (during treatment) when cysts are large. The leftover epithelium may give rise to the development of a new cyst.TREATMENT
OKCs are aggressive and have high recurrence rates (an average of 30%). It is thus very important to completely remove them.
Peripheral ostectomy along with chemical cauterization (Carnoy’s solution) of the bone after removal of the cyst is recommended.
Large OKCs can also be reduced in size by decompression and subsequently removed.
QUESTIONS? BRING 'EM ON!!
Orthokeratinized odontogenic cyst (OOC) is a variant of OKC. Is this true?
Would OKC show its characteristic histopathology picture if it was infected/inflamed?
Can OKC undergo a malignant transformation to squamous cell carcinoma?
The basal epithelial cells are cuboidal to columnar and palisaded, described as having a “tomb stone appearance”. Can you recollect any other lesion of the oral cavity, whose histology also shows basal cells having a tombstone appearance?
ANSWERS
Nope, OOC is not a variant of OKC!
Orthokeratinized odontogenic cyst (OOC) was first described as an orthokeratinizing variant of odontogenic keratocyst (OKC) in 1981. The basis of this distinction was the difference in its histopathology and its reduced chances of recurrence as compared to OKC.
It is now known and accepted that OOC is a distinct clinic-pathologic entity on its own. In fact it has been listed as a developmental odontogenic cyst in the recent (2017) WHO classification of odontogenic cysts.
It wouldn’t!
In the presence of intense inflammation, the overlying epithelium may lose its characteristic features, wherein parakeratinization and the palisading of basal layer are lost. Also, the epithelium may develop rete ridges. In such cases it would be difficult to make a diagnosis.
Yes, OKC has been reported to undergo malignant transformation to oral squamous cell carcinoma although very rarely.
The epithelium in pemphigus vulgaris shows acantholysis (loss of cohesion between the epithelial cells) in the parabasal layers with the basal layers being attached to the basement membrane. The basal cells resemble a “row of tombstones”.
✅HIGHLIGHTS - VIVA & ENTRANCE EXAM PERSPECTIVE
This cyst is believed to develop from --> a) from the rests of the dental lamina and b) extensions of the basal cells from the overlying epithelium (“basal cell hamartias” or “basal cell offshoots”).
OKC has an aggressive and destructive behaviour as compared to other odontogenic cysts. Also, some OKCs have been reported to have genetic mutations in the PTCH1 and P53 genes giving it a greater growth potential.
Predominantly occurs in the mandible usually in the third molar-ramus area.
A characteristic feature of OKC is its antero-posterior growth within the marrow cavity of the bone, causing no bone expansion despite its size.
OKC has been reported to be associated with nevoid basal cell carcinoma syndrome or Gorlin syndrome.
The epithelium does not have a prominent granular layer as present in orthokeratinized odontogenic cyst (OOC) (a factor differentiating OKC from OOC).
The fibrous wall/connective tissue may harbour satellite cysts, cords or islands of odontogenic epithelium.
OKC has a high recurrence rate (an average of 30%).
Incomplete removal of OKC may lead to development of new cysts due to the retained satellite cysts and odontogenic islands or rests in the cyst wall.
The epithelial lining is thin and friable, and may be difficult to completely remove (during treatment) when cysts are large. The leftover epithelium may give rise to the development of a new cyst.
Peripheral ostectomy along with chemical cauterization (Carnoy’s solution) of the bone after removal of the cyst is recommended.
📖REFERENCES AND FURTHER READING
Shear M, Speight PM. Cysts of the Oral and Maxillofacial Regions. 4 th ed. Blackwell Munksgaard; 2007.
Neville BW, Damm DD, Allen CM, Chi A. Oral and Maxillofacial Pathology. South Asian ed. Elsevier; 2016.
Rajendran R, Sivapathasundaram B. Shafer’s Textbook of Oral Pathology. 7th ed. Elsevier; 2012.
Regezzi JA, Sciubba JJ, Jordan RCK. Oral Pathology: Clinical Pathologic Correlations. 5 th ed. Elsevier; 2007.
Sapp JP, Eversole LR, Wysocki GP. Contemporary Oral and Maxillofacial Pathology. 2 nd ed. Mosby; 2004.
Speight PM, Takata T. New tumour entities in the 4th edition of the World Health Organization Classification of Head and Neck tumours: odontogenic and maxillofacial bone tumours. Virchows Arch. 2018 Mar;472(3):331-339.
MacDonald-Jankowski DS. Orthokeratinized odontogenic cyst: a systematic review. Dentomaxillofacial Radiology. 2010;39(8):455-467.