
Oral Epithelial Dysplasia (Notes & Video)

Certain red/white/red-white lesions of the oral cavity have a potential or a higher risk to develop malignancy (oral squamous cell carcinoma). Such lesions are called “Oral potentially malignant disorders (OPMD)”.
OPMDs may (or may not) show epithelial dysplasia histopathologically.
The term “dysplasia” denotes the abnormal development of a tissue and “epithelial dysplasia (ED)” is used to designate the atypical characteristics of the epithelium (indicating malignant risk) under the microscope.
ED is characterized by --> a) cellular atypia and b) disruption in the architectural orientation of the tissue.
💡UNDERSTANDING HOW EPITHELIAL DYSPLASIA WORKS
Cells, when insulted by carcinogens like tobacco would undergo damage that is initially reversible. This is a phase of adaptation by the cells and they would return to normalcy when the insult (tobacco) is removed. Also, any insult that could cause inflammation may cause the same pattern of reversible cell damage.
In the context of the oral epithelium being irritated by, let’s say tobacco, the initial reversible “adaptation” phase may manifest in the form of a hyperplasic epithelium and even mild atypical features.
Persistence of the tobacco habit may cause the epithelium to slip into a phase of irreversible cell damage. That is, cells do not revert to normalcy even after the removal of the irritant. The body’s usual response would be to get rid of the irreversibly damaged cells by apoptosis (homeostatic control). However, accumulated / induced mutations (due to tobacco) would help the damaged cells to persist (escape apoptosis) and proliferate. These are tumor cells and are histologically atypical. As more cells are affected there is a collective disruption of the tissue architecture. The tissue (epithelial layer) is now termed “dysplastic”.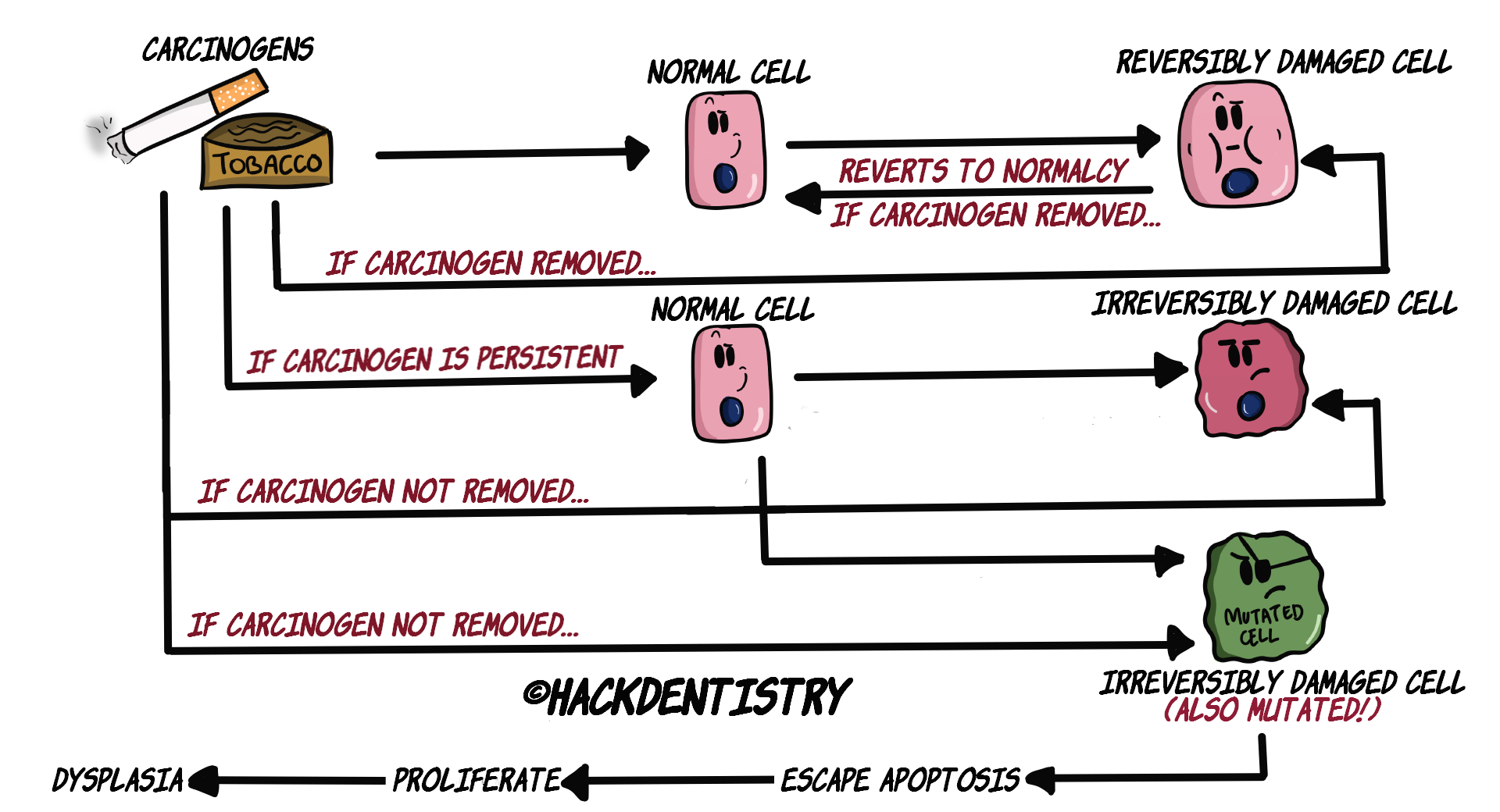
DIAGNOSTIC CRITERIA
Though there have been many proposed criteria to grade oral epithelial dysplasia (OED) since 1969, the WHO 2005 criteria came to be most widely followed.
Recently (2017), WHO published the grading system & criteria for OED, with minor changes to the criteria proposed in 2005.
Dysplasia is categorized as those affecting/disrupting the architecture of the epithelium and those changes manifesting as cellular atypia.
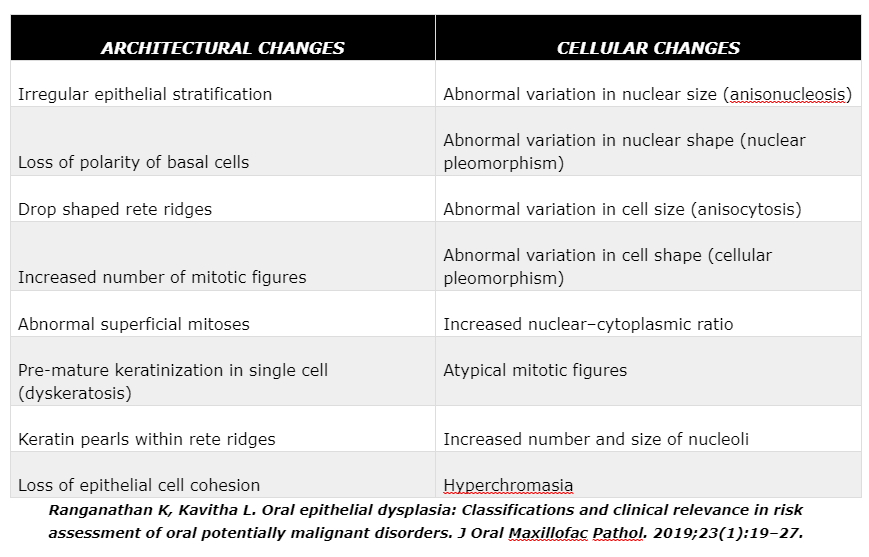
ARCHITECTURAL CHANGES
Irregular epithelial stratification --> The normal epithelium consists of tall basal cells which become larger and flatter in the upper most layers. However, cells in the upper layers of the dysplastic epithelium (spinous cells and above) may resemble basal cells. This is due to the inability of the basal cells to differentiate into the larger & flatter cells up in the epithelial strata.
Loss of polarity of basal cells --> Due to the excess proliferation of the basal cells, the basal layer becomes crowded and its orientation or orderly arrangement is lost.
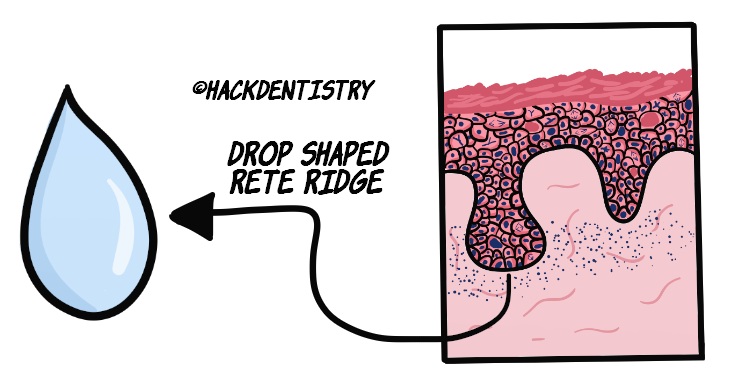
Drop shaped rete ridges --> The normal, long, tube shaped rete ridges become bulbous and drop shaped in a dysplastic epithelium.
Increased number of mitotic figures --> There is an increase in proliferation and hence an increase in the mitotic figures. However, note that normal epithelium as well as reactive lesions would also show mitotic figures in the basal and parabasal layers.

Abnormal superficial mitoses --> Of significance is the fact that dysplastic epithelium shows mitotic figures in all layers of the epithelium (unlike in the normal epithelium where mitotic figures are restricted to the basal and parabasal layers).
Dyskeratosis & keratin pearls --> Atypical epithelial cells may abnormally produce keratin within a single cell which is referred to as dyskeratosis. Numerous abnormal cells may produce abnormal keratin which accumulates in focal areas as pools of keratin. These foci of abnormal keratin are called keratin pearls.

Loss of epithelial cell cohesion --> Loss of cohesion between epithelial cells although rare may be present in severe epithelial dysplasia.
CELLULAR CHANGES
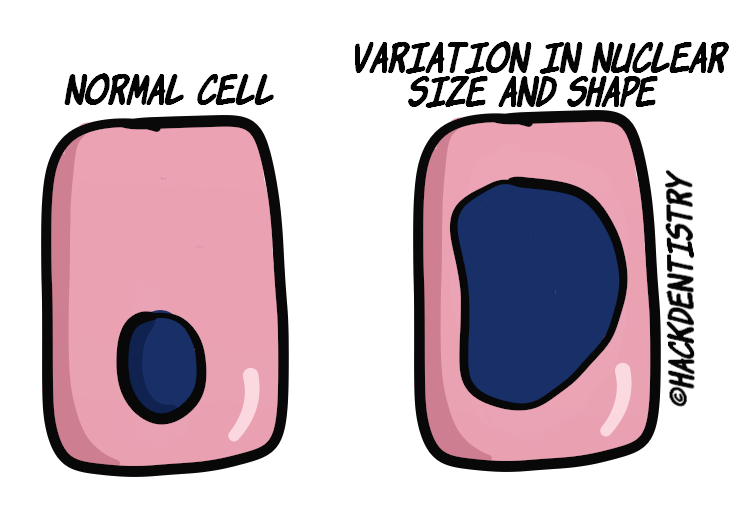
Variation in nuclear size & shape --> The nucleus becomes disproportionately large for the cell and the nuclear : cytoplasmic ratio is increased to 1:1 (as compared to 1:4 – 1:6 normally). The shape of the nucleus is irregular and may show coarse clumping of chromatin making
the nucleus appear hyperchromatic! Large nucleoli, often many in number, also appear in the nucleus.
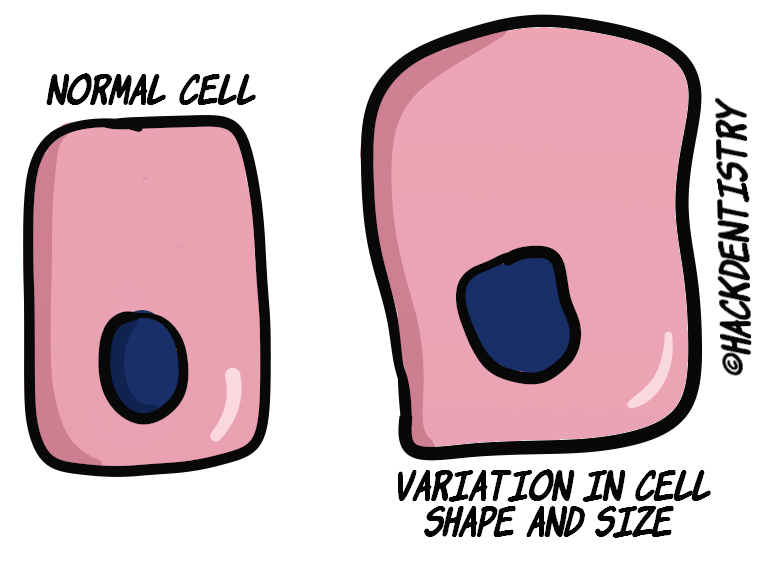
Variation in cell size & shape --> Similar to the nuclei, cells also show an abnormal variation in shape and size (pleomorphism).
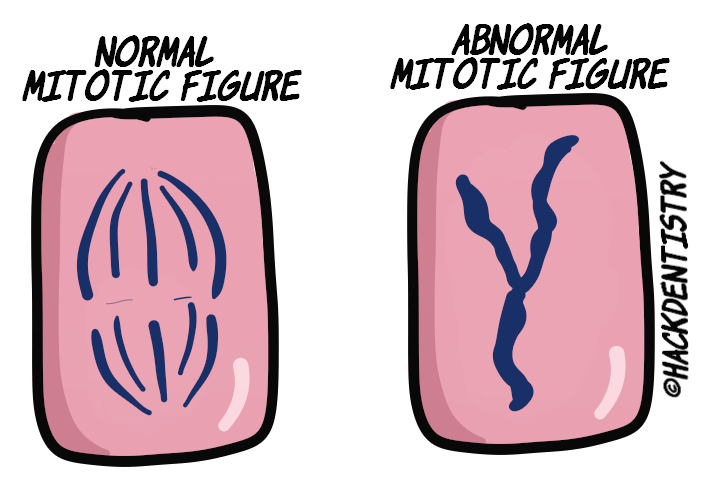
Atypical mitotic figures --> Mitotic figures are atypical/abnormal. They appear enlarged, tripolar and stellate shaped.
GRADING OF DYSPLASIA
WHO 2017 classification of OED advocates the grading of dysplasia as mild, moderate and severe.
Mild dysplasia --> defined when architectural disturbance is limited to the lower third of the epithelium with minimal cytological atypia.
Moderate dysplasia --> graded when architectural disturbance extends to the middle third of the epithelium with atypical cytological features being minimal. However if there is severe cellular atypia despite not extending beyond the middle third, it is justified to be graded severe.
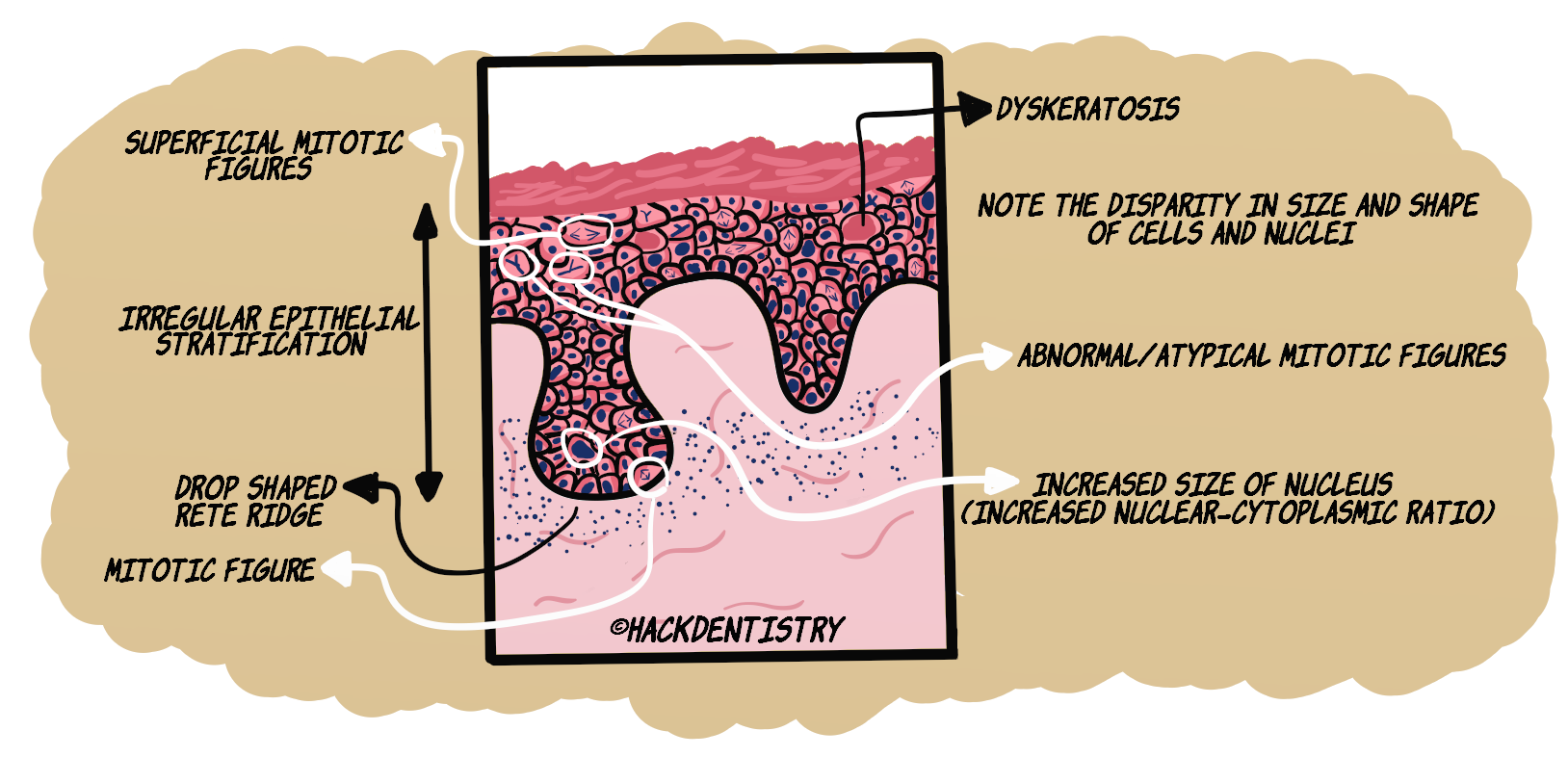
Severe dysplasia --> architectural changes extend to the full length of the epithelium together with cytological atypical features (see figure below).
💡RECENT UPDATES
In the 2005 WHO classification of OED, carcinoma in situ (CIS) meant the architectural changes extended to the full length (severe dysplasia --> upper 2/3rds) of the epithelium together with cytological atypical features. It was considered to be carcinoma with an absence of invasion/infiltration. The term CIS has however been removed from the 2017 WHO classification and has been clubbed with severe dysplasia.📷SEVERELY DYSPLASTIC EPITHELIUM
CLINICAL SIGNIFICANCE/OUTCOME
Assessing the presence and grading of epithelial dysplasia histologically, is still considered gold standard for predicting the malignant transformation of OPMDs.
In general lesions with mild dysplasia have better prognosis than those lesions with moderate or severe dysplasia.
Ironically, OPMD lesions without dysplasia may also rarely undergo malignant transformation.
Grading of epithelial dysplasia however, is subjective and may have considerable inter- and intra-observer variability.
✅HIGHLIGHTS - VIVA & ENTRANCE EXAM PERSPECTIVE
The term “dysplasia” denotes the abnormal development of a tissue and “epithelial dysplasia (ED)” is used to designate the atypical characteristics of the epithelium (indicating malignant risk) under the microscope.
ED is characterized by --> a) cellular atypia and b) disruption in the architectural orientation of the tissue.
Mild dysplasia --> defined when architectural disturbance is limited to the lower third of the epithelium with minimal cytological atypia.
Moderate dysplasia --> graded when architectural disturbance extends to the middle third of the epithelium with atypical cytological features being minimal. However if there is severe cellular atypia despite not extending beyond the middle third, it is justified to be graded severe.
Severe dysplasia --> architectural changes extend to the full length of the epithelium together with cytological atypical features.
Assessing the presence and grading of epithelial dysplasia histologically, is still considered gold standard for predicting the malignant transformation of OPMDs.
Ironically, OPMD lesions without dysplasia may also rarely undergo malignant transformation.
📖REFERENCES AND FURTHER READING
Rajendran R, Sivapathasundaram B. Shafer’s Textbook of Oral Pathology. 7th ed. Elsevier; 2012.
Ranganathan K, Kavitha L. Oral epithelial dysplasia: Classifications and clinical relevance in risk assessment of oral potentially malignant disorders. J Oral Maxillofac Pathol. 2019;23(1):19–27.
Warnakulasuriya S, Reibel J, Bouquot J, Dabelsteen E. Oral epithelial dysplasia classification systems: predictive value, utility, weaknesses and scope for improvement. J Oral Pathol Med. 2008;37(3):127-33.
Jerry E. Bouquot, Paul M. Speight, Paula M. Farthing.Epithelial dysplasia of the oral mucosa—Diagnostic problems and prognostic features.Current Diagnostic Pathology.2006;12: 11–21
Barnes L, Eveson JW, Reichart P, Sidransky S. World Health Organisation Classification of Tumours. Pathology and Genetics. Head and Neck Tumours. Lyon, France: International Agency for Research on Cancer Press; 2005.
Dionne KR, Warnakulasuriya S, Zain RB, Cheong SC. Potentially malignant disorders of the oral cavity: current practice and future directions in the clinic and laboratory. Int J Cancer. 2015 Feb 1;136(3):503-15.