
Tid Bits: Oral Potentially Malignant Disorders and Epithelial Dysplasia

Correction at 0:42 and 2:05 (Timestamps in video) - Oral precursor lesions were classified and defined as “Precancerous Lesions” and Precancerous Conditions” by a working group of the World Health Organization in 1978 (not 1972 as quoted in the video)
A reading of some of the lessons especially,
- Epithelial Dysplasia
- Erythroplakia
- Leukoplakia
- Oral Potentially Malignant Disorders
- Oral Squamous cell carcinoma
in the Chapter/Section "Epithelial Pathology" is recommended before jumping into this lesson.Q: What’s the deal with precancerous lesions, precancerous conditions and oral potentially malignant disorders? I am confused with these terms.
A: Certain red/white/red-white lesions of the oral cavity have a potential or a higher risk to develop malignancy (oral squamous cell carcinoma [OSCC]). Let us for the sake of clarity, understand that these lesions could be precursors to OSCC (note the word “could”, I’ll come back to this in a bit). In other words, these lesions or diseases could be defined as those that have altered the epithelium and have an increased likelihood of becoming cancer (OSCC).
Since they were “precursors” to cancer WHO in 1978 identified 2 types of oral diseases:
1) A “precancerous” lesion 👉 defined as “a morphologically altered tissue in which cancer is more likely to occur than in its apparently normal counterpart.”
2) A “precancerous” condition 👉 defined as “a generalised state associated with a significantly increased risk of cancer.’’
WHY CLASSIFY AS PRECANCEROUS LESIONS & CONDITIONS?
At that time this classification was not just academic. It was thought that malignancy (OSCC) occurring from a precancerous lesion, would appear in the same site as the precancer lesion. Eg - leukoplakia, erythroplakia
However, malignancy could develop anywhere in the oral cavity or pharynx if the individual suffered from a precancerous condition. Eg - oral lichen planus, oral submucous fibrosis.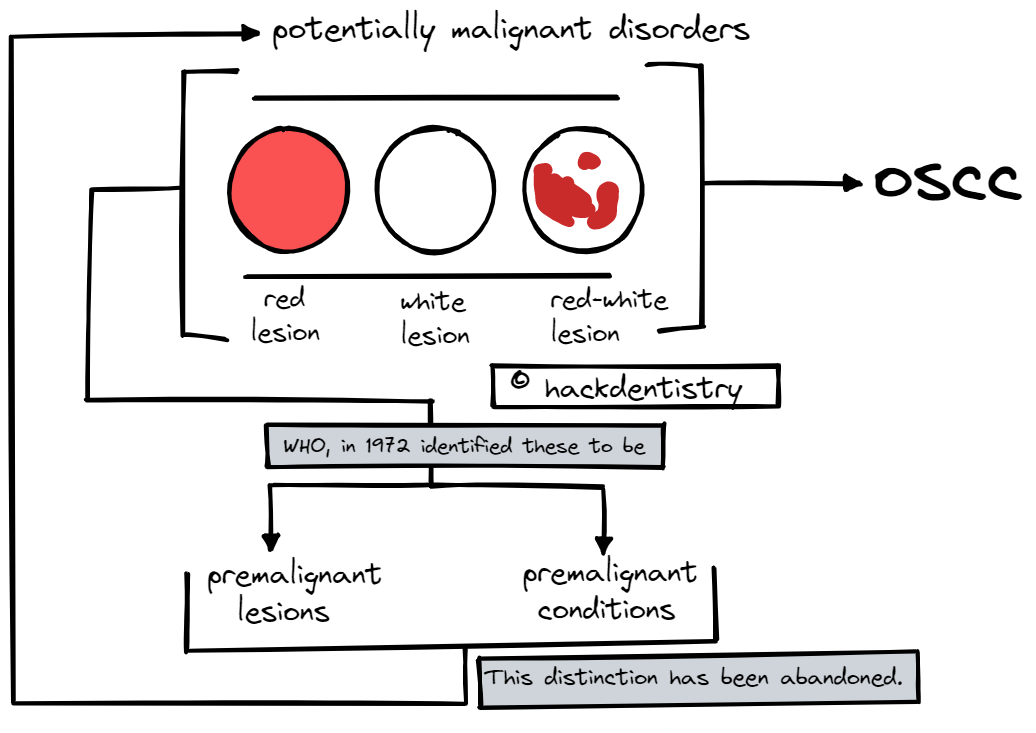
However, it was later understood that these lesions/conditions had only a “potential” risk to become cancer (the point I made above - certain red/white/red-white lesions “could” be precursors to OSCC). The malignant transformation was not inevitable. A patient with leukoplakia need not necessarily develop oral squamous cell carcinoma (OSCC). Moreover, it was also found that, for a patient with a defined lesion, such as leukoplakia, malignancy may arise elsewhere in the oral cavity (field cancerization theory). This is in opposition to the idea that OSCC would appear in the same site as the oral precancerous lesion.
These premises/arguments make the classification of these oral diseases as precancerous lesions and conditions redundant.
ORAL POTENTIALLY MALIGNANT DISORDERS
At a World Health Organization (WHO) workshop in 2005, it was recommended that the distinction between potentially malignant lesions and conditions be abandoned in favor of a common term, oral potentially malignant disorders (OPMDs) and this has now been accepted in the latest WHO classification.Q: Is epithelial dysplasia a significant predictor of malignant transformation of OPMDs?
A: It sort of “is” and “is not”. Before you get confused let me explain.
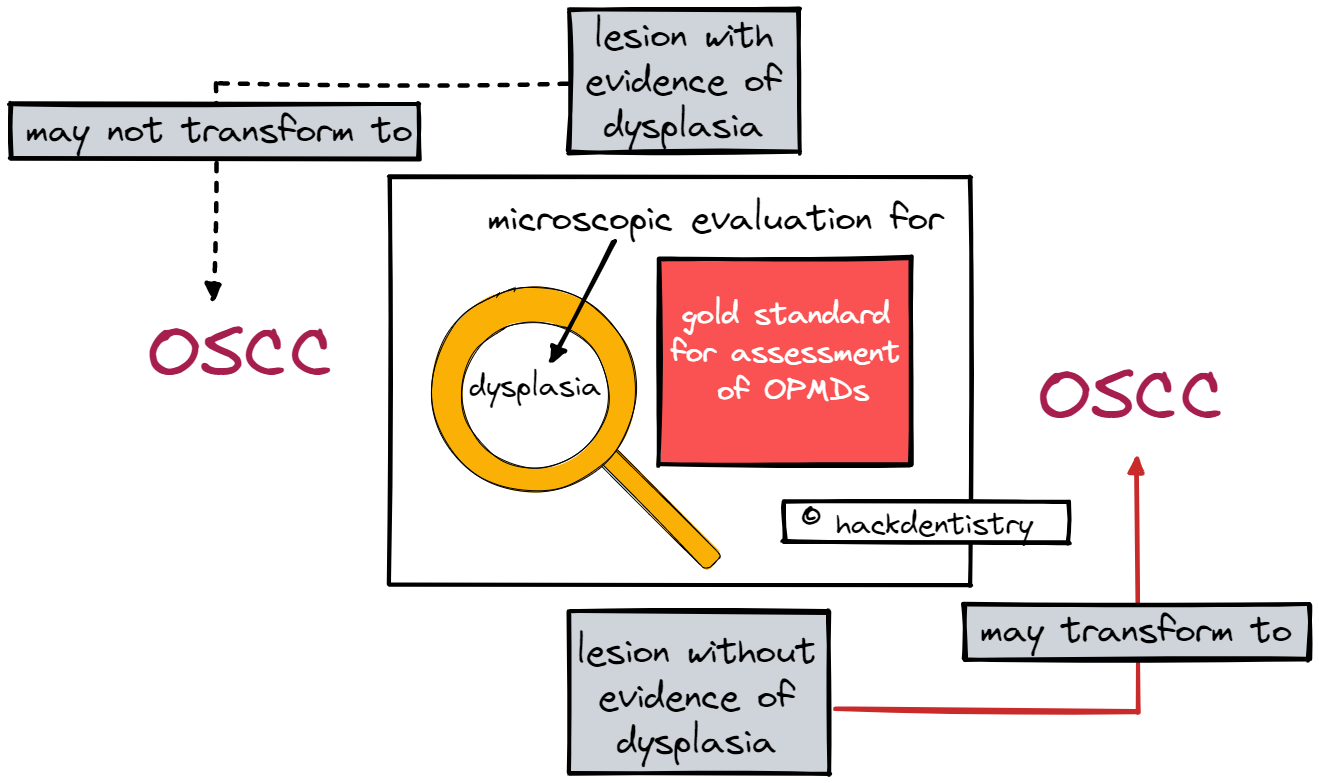
The microscopic evaluation for the presence of epithelial dysplasia in OPMDs remains the gold standard for the assessment of these lesions. It is believed that OPMDs with epithelial dysplasia have more chances of malignant transformation. Currently available molecular markers have not been proved to be of able predictors of malignant transformation.
However, it has to be remembered that it is not inevitable that a dysplastic lesion will transform into cancer. There is evidence of dysplastic lesions not progressing to carcinoma and also OPMDs without evidence of dysplasia progressing to cancer.
Q: Is Proliferative Verrucous Leukoplakia a distinct entity?
A: Proliferative verrucous leukoplakia(PVL) is considered to be a rare high risk form of leukoplakia (a variant of leukoplakia) first described by Hansen and associates in 1985.
This lesion manifests as an unsuspicious, homogenous white lesion in the early stages and does not show alarming features when biopsied. It starts to slowly spread to other areas of the oral cavity, becomes diffuse and multifocal, either confluent or isolated and surface of the lesion develops wart like projections to become verrucous. You could learn more about it here.
However, recent research suggests many differences including genomic differences to exist between PVL and standalone solitary leukoplakia, making it ripe for speculations if PVL in itself could be a distinct entity and not just a variant of leukoplakia.
Here are some differences:
1) PVL is usually large and multi-focal.
2) The recurrence rate for PVL is very high, between 70 - 100%.
3) There appears to be no correlation with alcohol consumption, tobacco chewing, smoking, or HPV infection.
4) There is a predilection for older females.
Q: Besides epithelial dysplasia, can the site and clinical appearance of an OPMD like leukoplakia be a predictor of malignant transformation?
A: Yes, they are significant predictors of malignant transformation.
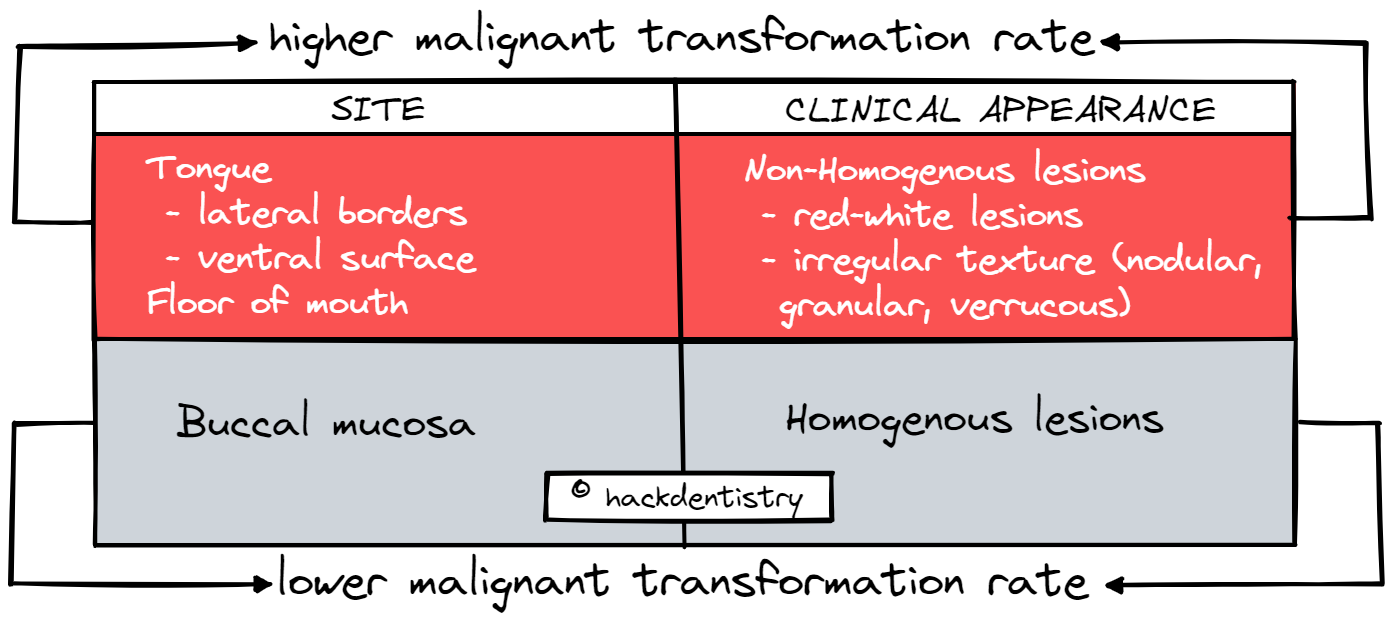
Site:
Lesions on the buccal mucosa have been found to have low malignant transformation rates. Whereas lesions on the lateral borders/ventral surface of the tongue and floor of the mouth have been found to have higher malignant transformation rates.
Clinical appearance:
Non-homogenous lesions (those that have both red and white components or those that have an irregular texture, like those that are nodular or verrucous) especially those white lesions that have red components have a higher malignant transformation rates that homogenous lesions. Research has shown that most early oral cancers, are red, or white lesions with red components.
REFERENCES AND FURTHER READING
Speight PM, Khurram SA, Kujan O. Oral potentially malignant disorders: risk of progression to malignancy. Oral Surg Oral Med Oral Pathol Oral Radiol. 2018 Jun;125(6):612-627.
Warnakulasuriya S, Johnson NW, van der Waal I. Nomenclature and classification of potentially malignant disorders of the oral mucosa. J Oral Pathol Med. 2007;36(10):575-80.
Sarode SC, Sarode GS, Tupkari JV. Oral potentially malignant disorders: A proposal for terminology and definition with review of literature. J Oral Maxillofac Pathol.2014 ;18(Suppl 1):S77-80.
Warnakulasuriya S. Clinical features and presentation of oral potentially malignant disorders. Oral Surg Oral Med Oral Pathol Oral Radiol. 2018 Jun;125(6):582-590
Küffer R, Lombardi T. Premalignant lesions of the oral mucosa. A discussion about the place of oral intraepithelial neoplasia (OIN). Oral Oncol. 2002 Feb;38(2):125-30
Woo SB. Oral Epithelial Dysplasia and Premalignancy. Head Neck Pathol. 2019;13(3):423-439.