
Oral squamous cell carcinoma - Clinical features and Histopathology (Note)

Oral squamous cell carcinoma (OSCC), very simply put, is a malignant neoplasm of the squamous cell or keratinocyte.
Various factors induce DNA mutations in the squamous cell, causing excess proliferation of these cells leading to cancer.
OSCC is known to be the most common oral malignancy. It is reported to account for 90% of all cancers occurring in oral cavity.
Very often, OSCC is preceded by oral potentially malignant disorders like leukoplakia or erythroplakia.
CLINICAL FEATURES
OSCC is reported to occur more commonly in older males (higher male predilection) in the lower socio-economic groups.
Though OSCCs could arise in a normal mucosa, most often they are preceded by potentially malignant disorders like leukoplakia, erythroplakia or mixed red-white lesions like speckled leukoplakia/leukoerythroplakia.
CLINICAL MANIFESTATIONS
OSCCs appear either as ulcerative lesions or exophytic lesions.
Ulcerative lesions may have rolled out borders or raised/exophytic margins.
Exophytic lesions (may be ulcerated too) appear verruciform or papillary.
Other clinical manifestations suggestive of OSCC
- red lesions suggestive of erythroplakia
- white lesions suggestive of leukoplakia
- mixed red-white lesions
- multifocal white or white-red lesions suggestive of proliferative verrucous leukoplakia
- lump on the oral mucosa
- a non healing extraction socketOSCC could appear in any site in the oral mucosa -> buccal mucosa, gingiva, tongue, floor of the mouth, lips and hard palate.
Buccal mucosa and gingiva -> OSCC occurs on this site usually in individuals with tobacco chewing habits. These individuals have a habit of pouching snuff in the gingivo-buccal sulcus leading to the lesion appearing in the associated buccal mucosa and gingiva.
Tongue -> the posterior lateral tongue and posterior one third of the tongue are usually affected. There is regional lymph node metastasis by the time the lesion is diagnosed. Prognosis is bad.
Floor of the mouth -> like the tongue, the prognosis for individuals with OSCC in this site is poor.
Lips -> lower lips are affected more frequently than the upper lip. The prognosis for OSCC on the lower lip is very good as compared to the upper lip which is worse.
Hard Palate -> very rare for OSCC to appear in this site. Individuals with the reverse smoking habit have their hard palate affected.
HISTOPATHOLOGY FEATURES
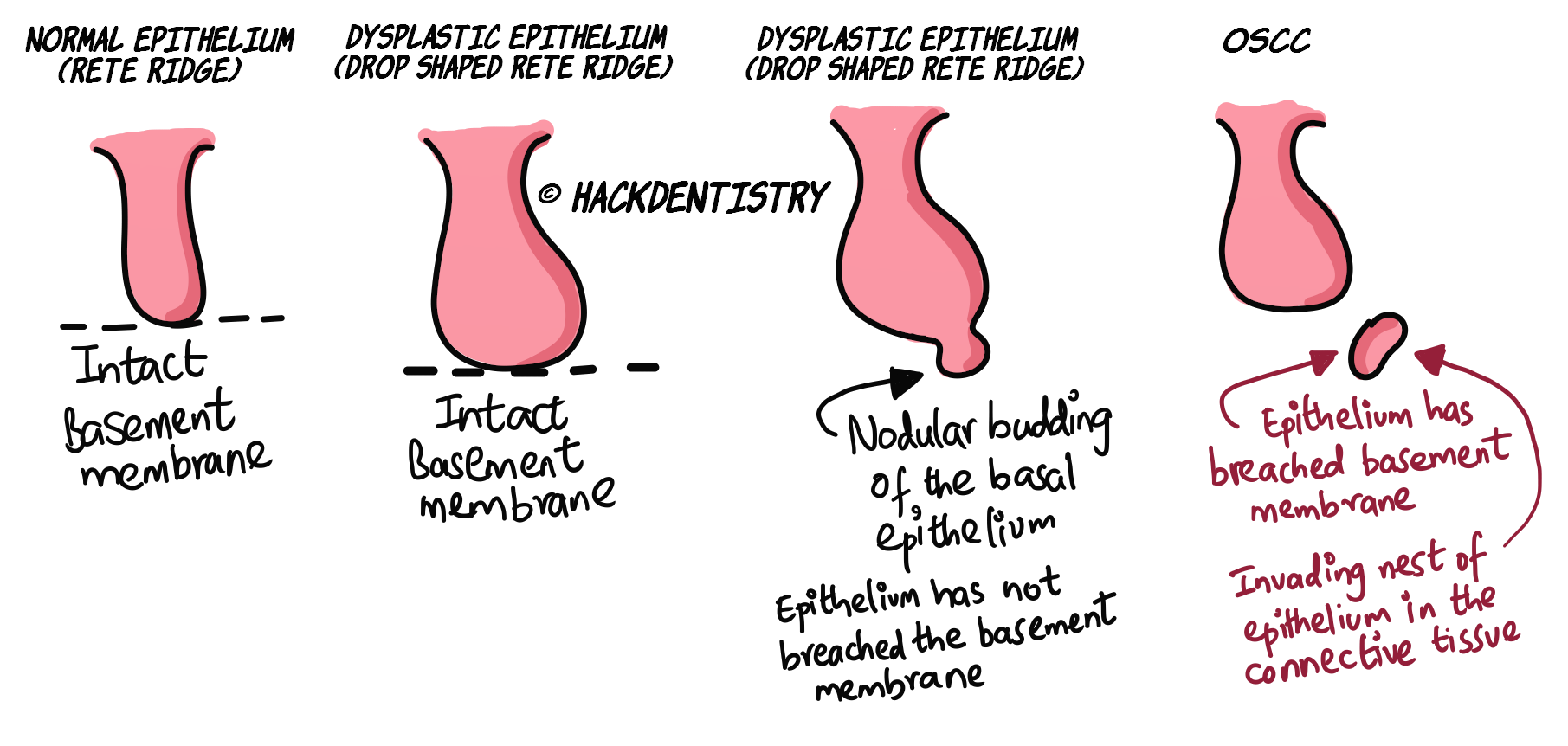
OSCC lesions are those in which the dysplastic epithelium has breached the basement membrane and invaded the connective tissue.
Strictly speaking even if a single cell breaches the basement membrane and invades the connective tissue, that lesion is considered to be carcinomatous.
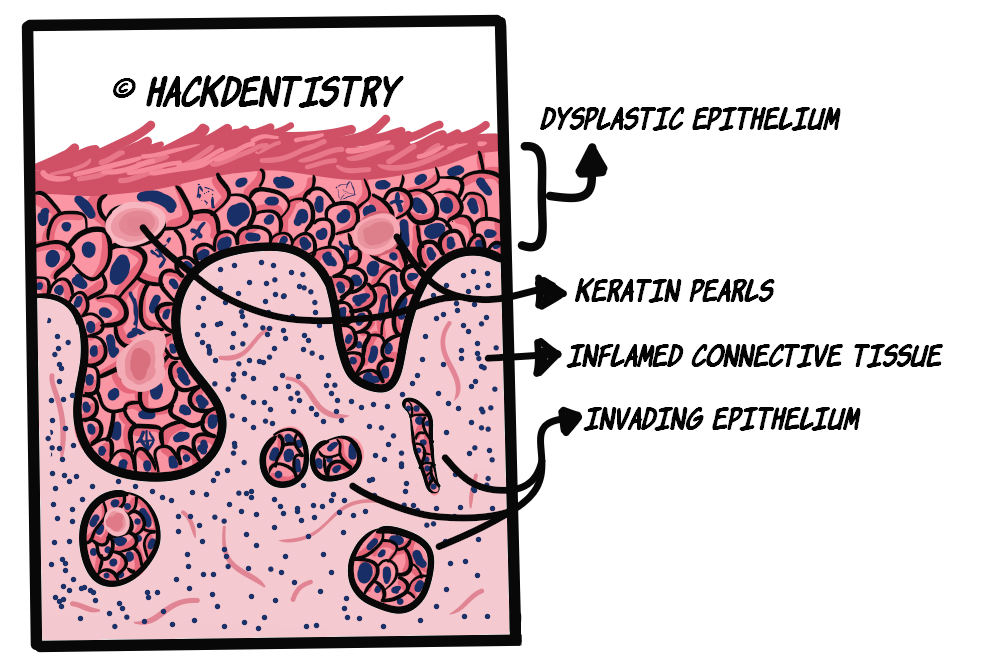
Under the microscope, the lesional tissue is dysplastic (read “epithelial dysplasia“) and shows cords, nests, islands or sheets of dysplastic squamous epithelium in the connective tissue.
The invading cords, nests or islands of malignant epithelial cells would extend deeply, penetrate and destroy other connective tissue components like adipose tissue, muscle, blood vessels or bone.
A characteristic feature of OSCC is the formation of keratin pearls and presence of individual cell keratinization.
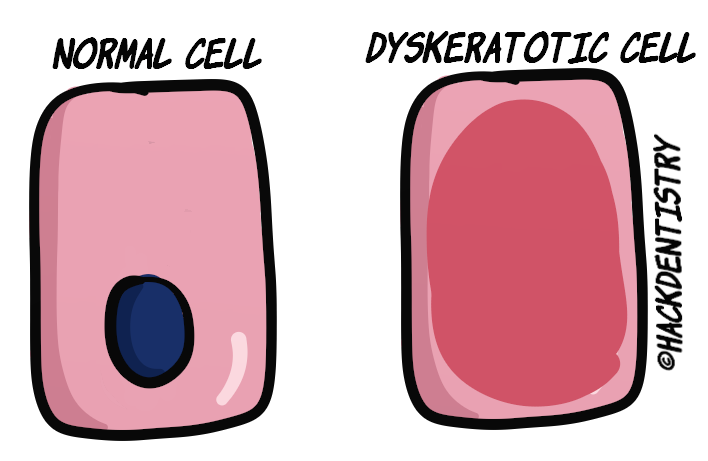
Atypical epithelial cells may abnormally produce keratin within a single cell which is referred to as dyskeratosis. Numerous abnormal cells may produce abnormal keratin which accumulates in focal areas as pools of keratin. These foci of abnormal keratin are called keratin pearls.
The connective tissue could show dense inflammation.
OSCC is graded as well, moderately and poorly differentiated based on its histologic resemblance to squamous epithelium.
Well-differentiated OSCC is easy to diagnose, very closely resembles squamous epithelium (tissue of origin). It usually shows numerous keratin pearls histologically. Squamous cells/keratinocytes produce keratin. Numerous abnormal cells (keratinocytes) may produce abnormal keratin which accumulates in focal areas as pools of keratin.
Cells in a poorly differentiated OSCC lesion would show marked pleomorphism to the extent of becoming anaplastic. They are very immature, show no keratinization or keratin pearls, and do not bear any resemblance to their tissue of origin. Such cases may need immunohistochemistry stains to identify the tissue of origin in order to diagnose the lesion.
Moderately differentiated OSCC lesions stand somewhere in between and show considerable pleomorphism, while also showing a few keratin pearls and some resemblance to the tissue of origin.
Among the 3 histologic grades, a well differentiated lesion has the best prognosis and a poorly differentiated tumor has the worst prognosis.
KNOW THY FACTS
Only when the epithelial cells have invaded the connective tissue is the lesion branded a “carcinoma”. A dysplastic epithelium without invasion is termed “epithelial dysplasia”.
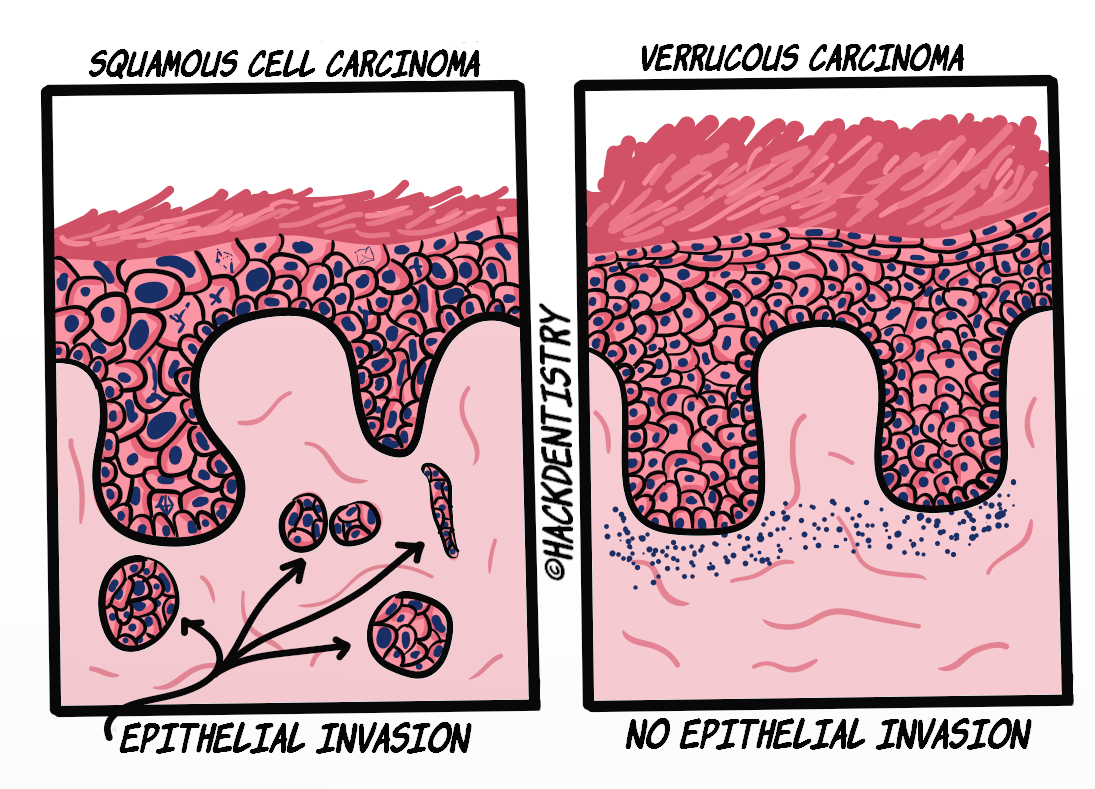
An exception to this rule is “Verrucous carcinoma” where there is no connective tissue invasion by the epithelium.
A BRIEF NOTE ON TNM STAGING
OSCC is staged based on 3 parameters, in order to predict the prognosis of the lesion.
The 3 parameters taken into account are:
Tumor size
Regional Lymph Node involvement
Distant Metastasis
These parameters are determined and are used for staging the tumor (OSCC lesion).
OSCC, based on the TNM staging, can be worked into 5 stages -> stage 0, through stage IV. The higher the stage of the tumor, the worse is its prognosis.
TREATMENT
OSCC, based on its size and site, is treated by surgical excision, radiation therapy or both.
Also based on regional lymph node involvement, it is treated with a combination of lymph node dissection.
Treatment and prognosis of OSCC depends on the site of the lesion, staging as well as the histologic grade.
HIGHLIGHTS - VIVA & ENTRANCE EXAM PERSPECTIVE
OSCC is known to be the most common oral malignancy. It is reported to account for 90% of all cancers occurring in oral cavity.
OSCC occurs on buccal mucosa and gingiva in individuals with tobacco chewing habits. These individuals have a habit of pouching snuff in the gingivo-buccal sulcus leading to the lesion appearing in the associated buccal mucosa and gingiva.
OSCC lesions are those in which the dysplastic epithelium has breached the basement membrane and invaded the connective tissue.
Under the microscope, the lesional tissue is dysplastic (read “epithelial dysplasia“) and shows cords, nests, islands or sheets of dysplastic squamous epithelium in the connective tissue.
A characteristic feature of OSCC is the formation of keratin pearls and presence of individual cell keratinization.
OSCC is graded as well, moderately and poorly differentiated based on its histologic resemblance to squamous epithelium.
Among the 3 histologic grades, a well differentiated lesion has the best prognosis and a poorly differentiated tumor has the worst prognosis.
QUESTIONS? BRING ‘EM ON!!
Q: A 63 year old male was clinically diagnosed with verrucous leukoplakia. A biopsy was done and the histopathology report was as follows:
“The H & E stained section shows hyperkeratotic parakeratinized hyperplastic stratified squamous epithelium with exophytic projections, overlying a densely inflamed stroma. The epithelium shows clefts with keratin plugging in several areas and broad bulbous rete ridges with an endophytic growth pattern. The connective tissue shows dense inflammation with focal areas of nests and islands of dysplastic epithelial cells.”
What would be the most likely diagnosis (refer the histopathology section for clues)??
ANSWER
The lesion should be diagnosed as squamous cell carcinoma!
The biopsy report revealed the lesion had all features diagnostic of verrucous carcinoma. Diagnosis of verrucous carcinoma is confirmed, when the broad rete ridges show an endophytic growth, i.e, the lesional rete ridges “push” into the connective tissue with an intact basement membrane, beyond the adjacent basement membrane of the normal epithelium.
However, note the last line of the report which says “The connective tissue shows focal areas of nests and islands of dysplastic epithelial cells”. Verrucous carcinoma does not show invasion of epithelial cells into the connective tissue unlike squamous cell carcinoma. In fact, it is important for pathologists to screen the lesion thoroughly, to check for foci of conventional squamous cell carcinomas within a verrucous carcinoma. Foci of invading dysplastic epithelial islands in the connective tissue should raise a “red flag” and such lesions should be diagnosed and treated as conventional squamous cell carcinomas.
REFERENCES AND FURTHER READING
Scully C, Bagan J. Oral squamous cell carcinoma overview. Oral Oncol. 2009;45(4-5):301-308.
Pires FR, Ramos AB, Oliveira JB, Tavares AS, Luz PS, Santos TC. Oral squamous cell carcinoma: clinicopathological features from 346 cases from a single oral pathology service during an 8-year period. J Appl Oral Sci. 2013;21(5):460-467.
Sanketh DS, Patil S, Rao RS. Estimating the frequency of Candida in oral squamous cell carcinoma using Calcofluor White fluorescent stain. J Investig Clin Dent. 2016;7(3):304-307.
Neville BW, Damm DD, Allen CM, Chi A. Oral and Maxillofacial Pathology. South Asian ed. Elsevier; 2016.
Rajendran R, Sivapathasundaram B. Shafer’s Textbook of Oral Pathology. 7th ed. Elsevier; 2012.
Regezzi JA, Sciubba JJ, Jordan RCK. Oral Pathology: Clinical Pathologic Correlations. 5 th ed. Elsevier; 2007.
Sapp JP, Eversole LR, Wysocki GP. Contemporary Oral and Maxillofacial Pathology. 2 nd ed. Mosby; 2004.