
Oral squamous cell carcinoma - Etiology and Pathogenesis (Note and Video)

Oral squamous cell carcinoma (OSCC), very simply put, is a malignant neoplasm of the squamous cell or keratinocyte.
Various factors induce DNA mutations in the squamous cell, causing excess proliferation of these cells leading to cancer.
OSCC is known to be the most common oral malignancy. It is reported to account for 90% of all cancers occurring in oral cavity.
Very often, OSCC is preceded by oral potentially malignant disorders like leukoplakia or erythroplakia.
ETIOLOGY
OSCC is known to have a multifactorial etiology. There are many factors that could possibly lead to causing OSCC.
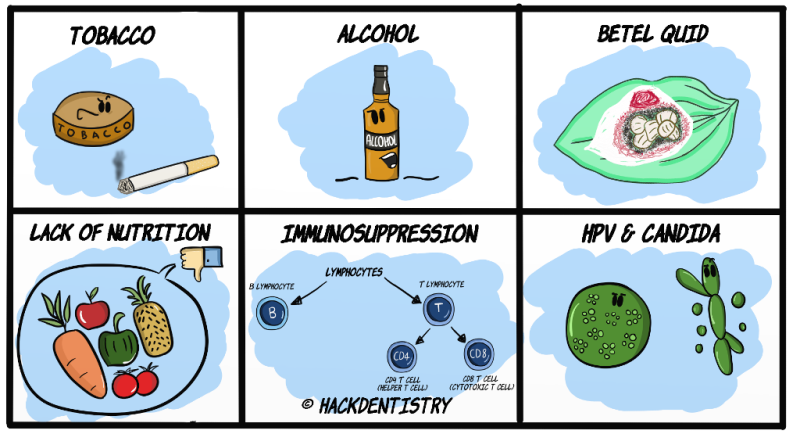
Tobacco (smoking and smokeless)
Both tobacco smoking and smokeless tobacco are regarded to be strongly linked to cause OSCC. In fact, majority of individuals with OSCC are known to have a smoking habit.
Pipe and cigar smoking are reported to be riskier than cigarette smoking when it comes to causing OSCC. Pipe smokers have a strong predilection for squamous cell carcinoma of the lower lip.
Bidi smoking, prevalent in places like India, is known to be 3 times riskier than cigarette smoking.
A deleterious habit called “Reverse smoking”, where the smoker keeps the lighted end of the cigarette inside the mouth, is known to have the highest risk of causing OSCC. In these cases, it is the hard palate that is usually affected.
Other habits like chewing dry/wet snuff and tobacco pouching are also known to cause OSCC.
💡KNOW THY FACTS
Tobacco smoking or chewing, is the most common etiologic factor in causing OSCC in places like India. Most commonly, tobacco habits lead to causing oral potentially malignant disorders like leukoplakia, erthroplakia, leuko-erythroplakia and submucous fibrosis. Though not all of them transform, they have the potential to become malignant. Most cases of OSCC are preceded by dysplastic potentially malignant disorders.Alcohol
Though it does not have a direct correlation, alcohol is reported to work in synergy with tobacco in causing OSCC.
Alcohol in combination with tobacco is a considerable risk factor.
Betel quid
Betel quid consists of a betel leaf that wraps a mixture of arecanut, slaked lime (calcium hydroxide), tobacco and other spices.
Betel quid chewing is mainly implicated in causing oral submucous fibrosis (OSF). However, it is also reported that, arecoline (an alkaloid of arecanut) can induce carcinogenesis.
Moreover, OSF is classified as a potentially malignant disorder and is estimated to have a 7-13% rate of malignant transformation to OSCC.
Nutritional deficiencies
High fat and sugar intake, with low fruits and vegetable intake has been implicated to be a risk factor.
Low levels of Vitamin A and C.
Plummer-Vinson syndrome (also called Paterson-Kelly syndrome) is one of the most significant manifestations of iron deficiency anemia. It predisposes an individual to pharyngeal or esophageal squamous cell carcinoma.
Immunosuppression
Patients with a compromised immune system have considerable risk in developing OSCC.
HIV/AIDS patients --> increased risk of oral cancer.
Patients whose immune systems are suppressed for bone marrow or organ transplant (kidney) have been reported to develop oral cancer.
HPV and Candida
A number of studies have reported Human Papilloma Virus (HPV) to be associated with oro-pharyngeal carcinomas.
Certain strains of Candida albicans are known to produce N-nitrosobenzylmethylamine, which is a carcinogen. It has been reported that these products either directly or in association with other carcinogens could induce OSCC.
A clinical type of candidal lesion called Hyperplastic candidiasis (previously called chonic hyperplastic candidiasis) is known to manifest with dysplasia histologically.
💡KNOW THY FACTS
There are reports that state candida organisms could induce hyperplasia and cause hyperkeratotic white lesions. Hence, some pathologists and investigators believe hyperplastic candidiasis could cause dysplastic leukoplakic lesions and regard them as being potentially malignant.
However, there are researchers who doubt this condition could arise as a result of candida and believe it to be a “candidal infection superimposed on a pre-existing leukoplakic lesion”.PATHOGENESIS
The above listed etiologic factors or mutagens (especially tobacco and betel quid) could cause genetic alterations/mutations of the squamous cell, that alter their biologic behavior.
Accumulated/induced mutations help the damaged cells to persist (escape apoptosis) and proliferate (read more on this in the lesson “Oral Epithelial Dysplasia“).
At this stage mutated squamous cells are tumor cells and are histologically atypical (dysplastic).
Usually there is a healthy balance of cell proliferation (induced by oncogenes) and cell cycle arrest (by tumor suppressor genes). Mutations accumulating in oncogenes and tumor suppressor genes result in altered cell behavior and carcinogenesis.
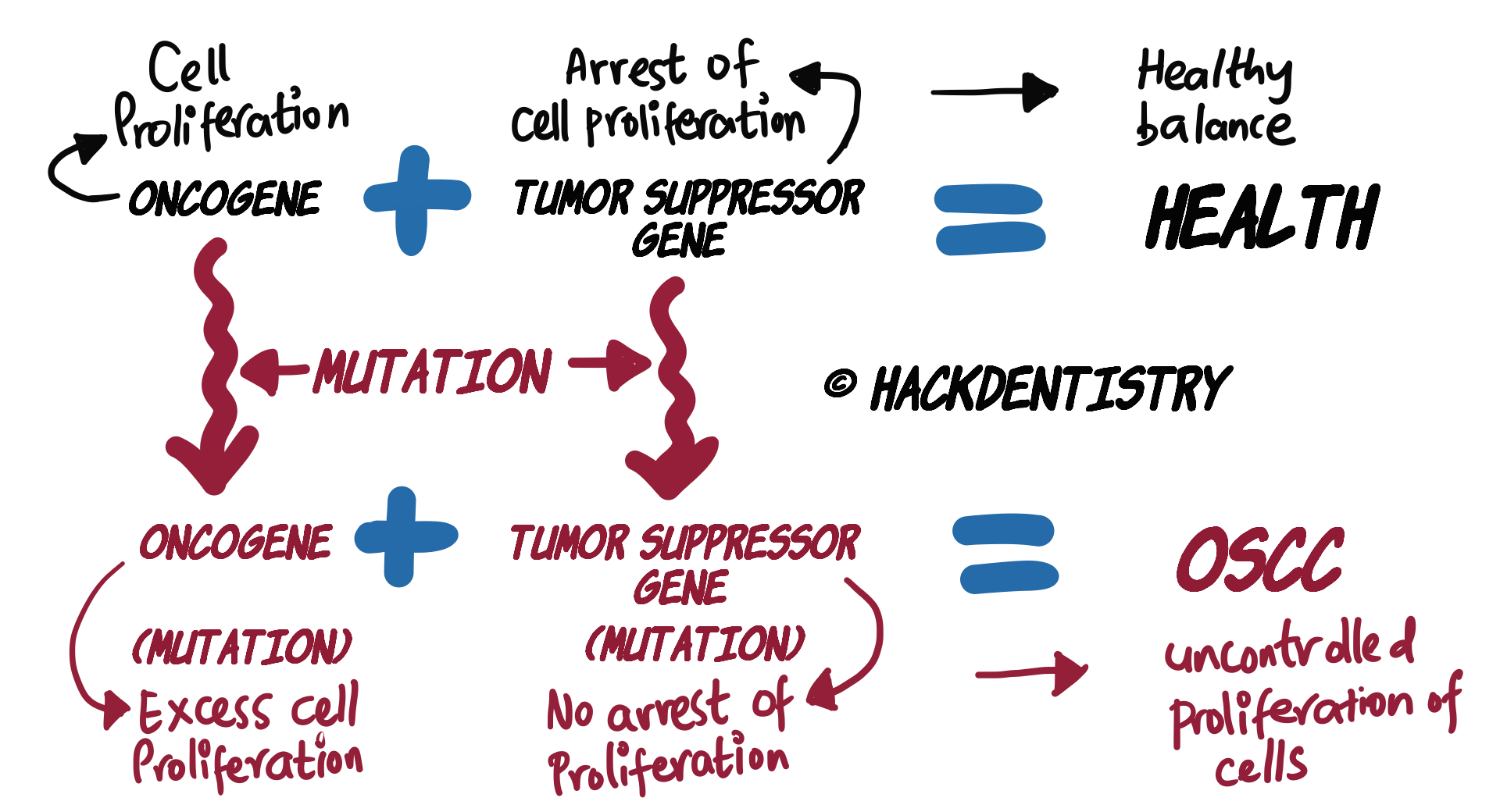
Oncogenes
Oncogenes are proteins that help cells proliferate.
Mutations in oncogenes could cause uncontrolled proliferation of cells.
Tumor suppressor genes
Tumor suppressor genes are proteins that help arrest the cell cycle (proliferation) and also cause apoptosis of the cell when necessary.
Mutations in tumor suppressor genes (usually p16, p53 and p21) could cause uncontrolled proliferation of cells (since mutations cause the tumor suppressor genes from functioning properly, thus indirectly helping proliferation).
HIGHLIGHTS - VIVA & ENTRANCE EXAM PERSPECTIVE
OSCC is known to be the most common oral malignancy. It is reported to account for 90% of all cancers occurring in oral cavity.
Pipe smokers have a strong predilection for squamous cell carcinoma of the lower lip.
A deleterious habit called “Reverse smoking”, where the smoker keeps the lighted end of the cigarette inside the mouth, is known to have the highest risk of causing OSCC.
Alcohol in combination with tobacco is a considerable risk factor.
Betel quid chewing is mainly implicated in causing oral submucous fibrosis (OSF). However, it is also reported that, arecoline (an alkaloid of arecanut) can induce carcinogenesis.
Plummer-Vinson syndrome (also called Paterson-Kelly syndrome) is one of the most significant manifestations of iron deficiency anemia. It predisposes an individual to pharyngeal or esophageal squamous cell carcinoma.
A number of studies have reported Human Papilloma Virus (HPV) to be associated with oro-pharyngeal carcinomas.
Certain strains of Candida albicans are known to produce N-nitrosobenzylmethylamine, which is a carcinogen. It has been reported that these products either directly or in association with other carcinogens could induce OSCC.
Usually there is a healthy balance of cell proliferation (induced by oncogenes) and cell cycle arrest (by tumor suppressor genes). Mutations accumulating in oncogenes and tumor suppressor genes result in altered cell behavior and carcinogenesis.
QUESTIONS? BRING 'EM ON!!
Note: Reading the next part of this lesson (Oral squamous cell carcinoma - Clinical features and Histopathology could help you answer this question)
Q: A 63 year old male was clinically diagnosed with verrucous leukoplakia. A biopsy was done and the histopathology report was as follows:
“The H & E stained section shows hyperkeratotic parakeratinized hyperplastic stratified squamous epithelium with exophytic projections, overlying a densely inflamed stroma. The epithelium shows clefts with keratin plugging in several areas and broad bulbous rete ridges with an endophytic growth pattern. The connective tissue shows dense inflammation with focal areas of nests and islands of dysplastic epithelial cells.”
What would be the most likely diagnosis (refer the histopathology section for clues)??
ANSWER
The lesion should be diagnosed as squamous cell carcinoma!
The biopsy report revealed the lesion had all features diagnostic of verrucous carcinoma. Diagnosis of verrucous carcinoma is confirmed, when the broad rete ridges show an endophytic growth, i.e, the lesional rete ridges “push” into the connective tissue with an intact basement membrane, beyond the adjacent basement membrane of the normal epithelium.
However, note the last line of the report which says “The connective tissue shows focal areas of nests and islands of dysplastic epithelial cells”. Verrucous carcinoma does not show invasion of epithelial cells into the connective tissue unlike squamous cell carcinoma. In fact, it is important for pathologists to screen the lesion thoroughly, to check for foci of conventional squamous cell carcinomas within a verrucous carcinoma. Foci of invading dysplastic epithelial islands in the connective tissue should raise a “red flag” and such lesions should be diagnosed and treated as conventional squamous cell carcinomas.
REFERENCES AND FURTHER READING
Scully C, Bagan J. Oral squamous cell carcinoma overview. Oral Oncol. 2009;45(4-5):301-308.
Pires FR, Ramos AB, Oliveira JB, Tavares AS, Luz PS, Santos TC. Oral squamous cell carcinoma: clinicopathological features from 346 cases from a single oral pathology service during an 8-year period. J Appl Oral Sci. 2013;21(5):460-467.
Sanketh DS, Patil S, Rao RS. Estimating the frequency of Candida in oral squamous cell carcinoma using Calcofluor White fluorescent stain. J Investig Clin Dent. 2016;7(3):304-307.
Neville BW, Damm DD, Allen CM, Chi A. Oral and Maxillofacial Pathology. South Asian ed. Elsevier; 2016.
Rajendran R, Sivapathasundaram B. Shafer’s Textbook of Oral Pathology. 7th ed. Elsevier; 2012.
Regezzi JA, Sciubba JJ, Jordan RCK. Oral Pathology: Clinical Pathologic Correlations. 5 th ed. Elsevier; 2007.
Sapp JP, Eversole LR, Wysocki GP. Contemporary Oral and Maxillofacial Pathology. 2 nd ed. Mosby; 2004.