
Oral submucous fibrosis (Note & Video)

Oral submucous fibrosis (OSF) is a chronic debilitating and scarring disease of the oral mucosa that is potentially malignant.
It is a condition characterized by an altered collagen metabolism which results in dense fibrosis of the oral cavity.
OSF was first described by Schwartz in 1952, and was then termed “atrophica idiopathica mucosae oris”. It was later renamed as OSF by Joshi 1953.
OSF is rare in the western countries and is most prevalent in India and South-East Asia.
ETIOLOGY & PATHOGENESIS
The main etiology for OSF is known to be betel quid chewing.
The dense fibrosis caused in this condition is due to the presence of arecanut in betel quid.
💡KNOW THY FACTS!
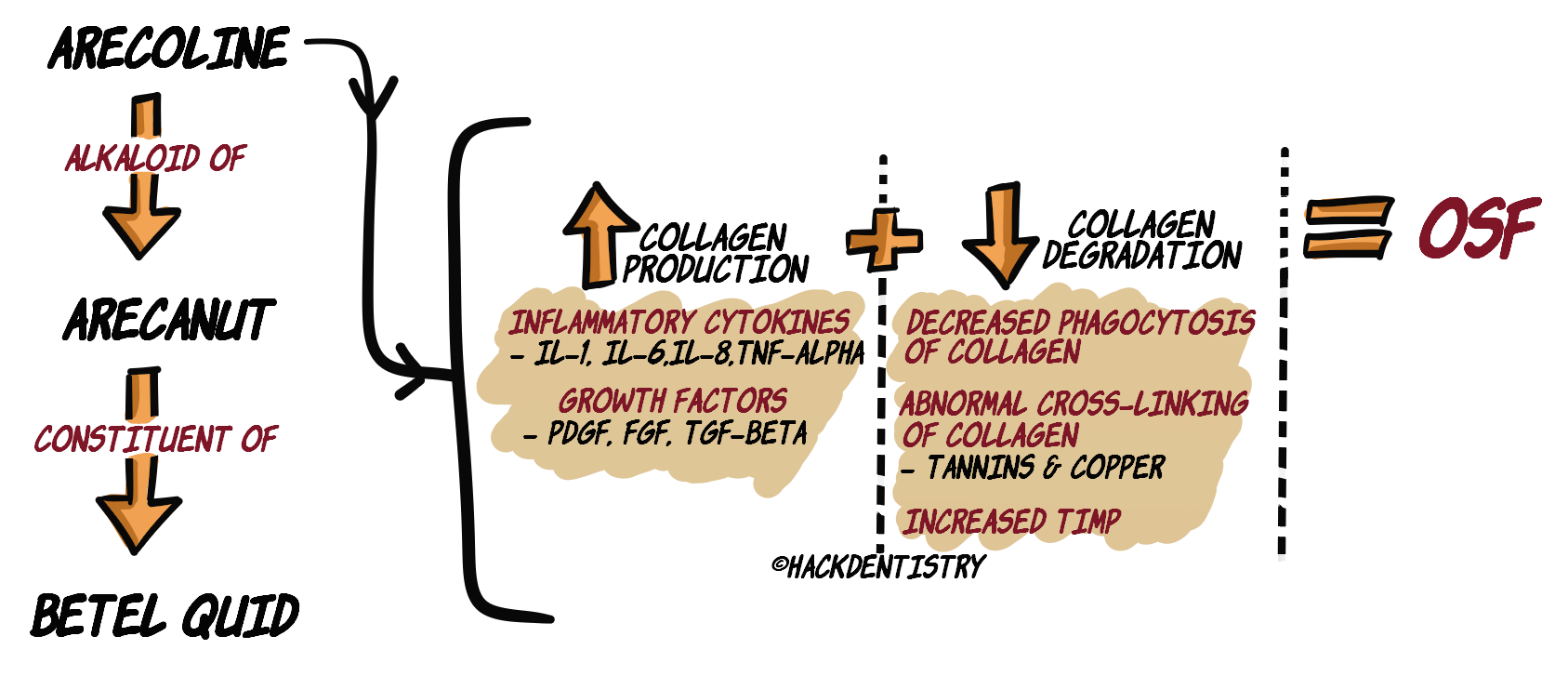
Betel quid consists of a betel leaf that wraps a mixture of arecanut, slaked lime (calcium hydroxide), tobacco and other spices. Other freeze-dried betel quid substitutes are pan masala, gutkha and mawa. The main constituent known to induce OSF is the arecanut present in betel quid and its substitutes.There has been sufficient research hypothesizing arecoline, an alkaloid of arecanut, to cause a disruption in the collagen metabolism that potentially leads to OSF.
INCREASED PRODUCTION OF COLLAGEN
Arecoline induces inflammatory cells to produce cytokines --> IL-1, IL-6, IL-8 and TNF-α. These cytokines can cause fibroblasts to increase collagen production.
Arecoline could upregulate the production of growth factors --> PDGF, TGF-β and FGF, which cause fibroblast to increase collagen production.
DECREASED DEGRADATION OF COLLAGEN
Arecoline could cause a reduction in phagocytic removal of collagen. This could cause decreased degradation of collagen.
Tannins (polyphenol) and copper in arecanut cause an increase in enzyme, lysyl oxidase --> causes abnormal cross-linking of collagen molecules --> decreased degradation of collagen.
Matrix metalloproteinase (MMP) degrades collagen; Tissue inhibitors of matrix metalloproteinases (TIMP) inhibit action of MMPs. Arecoline disturbs the balance between MMPs & TIMPs tipping it in the favour of TIMP. Increase in TIMP --> inhibition of MMP --> decreased collagen degradation.
OTHER FACTORS
Nutritional deficiencies like iron and vitamin B complex deficiency, as well as malnutrition could be promoting factors of the disease.
Genetic and molecular alterations have also been reported to contribute to pathogenesis of the disease.
CLINICAL FEATURES
Prevalent in India and South-East Asia usually in individuals between 40-60 years.
There has been an increase in the younger population affected by this disease (could be due to increase in adverse habits among the young).
A general female predilection has been reported though certain reports show a male predominance.
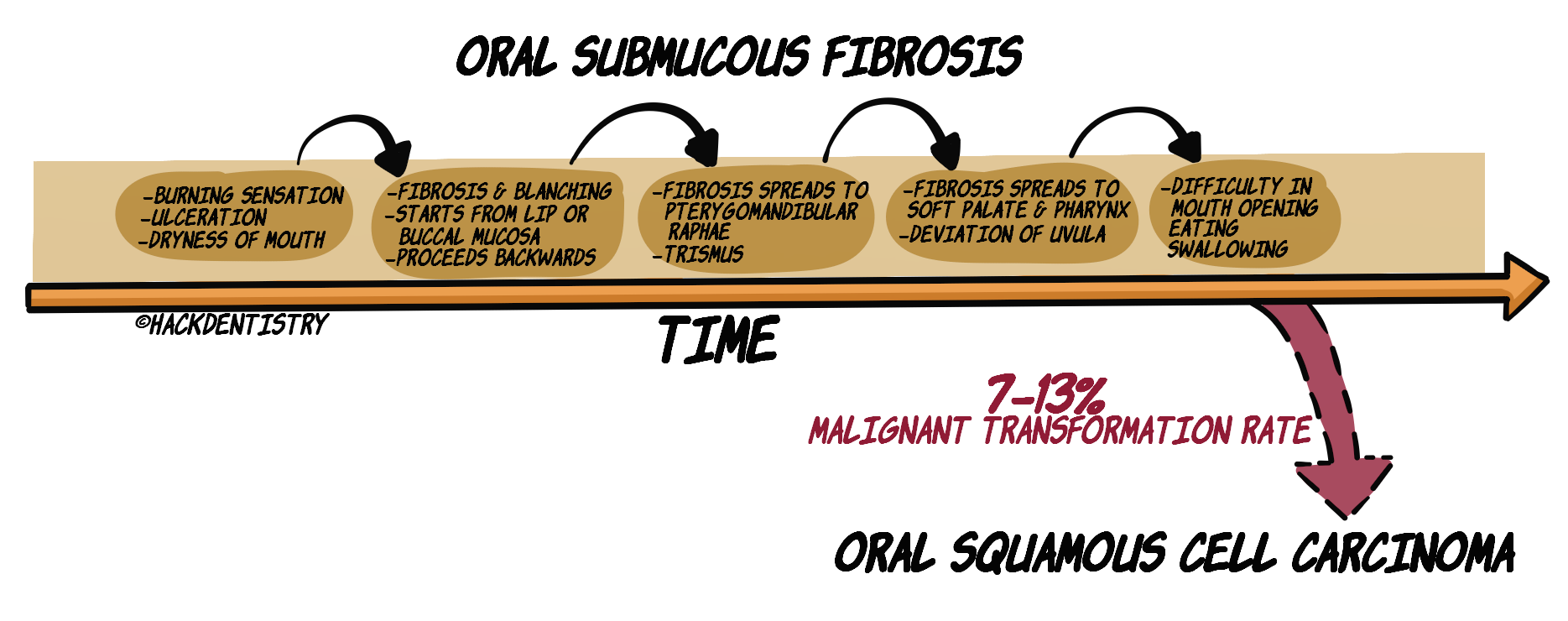
Early symptoms of OSF include a) burning sensation of the mouth (stomatopyrosis), b) appearance of blisters, ulcerations in the oral cavity and c) dryness of mouth.
OSF progresses to increased fibrosis --> blanching of oral mucosa.
Blanching starts from the lips or buccal mucosa and proceeds backwards.
Fibrous bands can be palpated (in tissues affected), usually running vertically.
Fibrosis spreads to the pterygomandibular raphae --> decreased mouth opening – trismus.
Advanced cases of OSF may have mouth opening reduced to <15mm (normal mouth opening – 39-70 mm for male; 36-56mm for female).
Fibrosis could also spread to the soft palate (causes deviation of uvula) and up to the pharynx.
OSF patients find it difficult to open their mouth, eat, swallow and whistle/blow.
💡KNOW THY FACTS!
- Betel quid chewing, apart from causing OSF is also known to cause other potentially malignant disorders like leukoplakia, verrucous hyperplasia and verrucous carcinoma. This is primarily due to the tobacco present in the betel quid, although it is also reported that arecoline can induce carcinogenesis.
- Another interesting lesion caused due to betel quid chewing is the oral lichenoid lesion appearing in tissues directly in contact with the betel quid.These lesions may present as fine white wavy, parallel striae and may sometimes radiate from a central erythematous area.MALIGNANT POTENTIAL OF OSF
OSF is classified as a potentially malignant disorder and is estimated to have a 7-13% rate of malignant transformation to oral squamous cell carcinoma (OSCC).
a) Dense fibrosis, b) lack of vascularity c) altered cytokines in the tissues of patients with OSF provides for a unique environment conducive for tobacco and arecanut to induce carcinogenesis.
HISTOPATHOLOGY FEATURES
EARLY STAGE
Epithelium shows flattening of rete ridges.
Juxta-epithelial hyalinization --> glassy, homogenous eosinophilic material deposited in connective tissue immediately below epithelium.
Presence of moderate numbers of plump fibroblasts.
Dilated and congested blood vessels in connective tissue.
Sparse inflammation usually lymphocytes and occasional plasma cells.
MODERATELY ADVANCED STAGE
Epithelium loses rete ridges, is markedly atrophic.
Moderately hyalinized collagen in connective tissue (due to increasing fibrosis).
Blood vessels begin to constrict.
Inflammatory infiltrate consists of lymphocytes, plasma cells and few eosinophils.
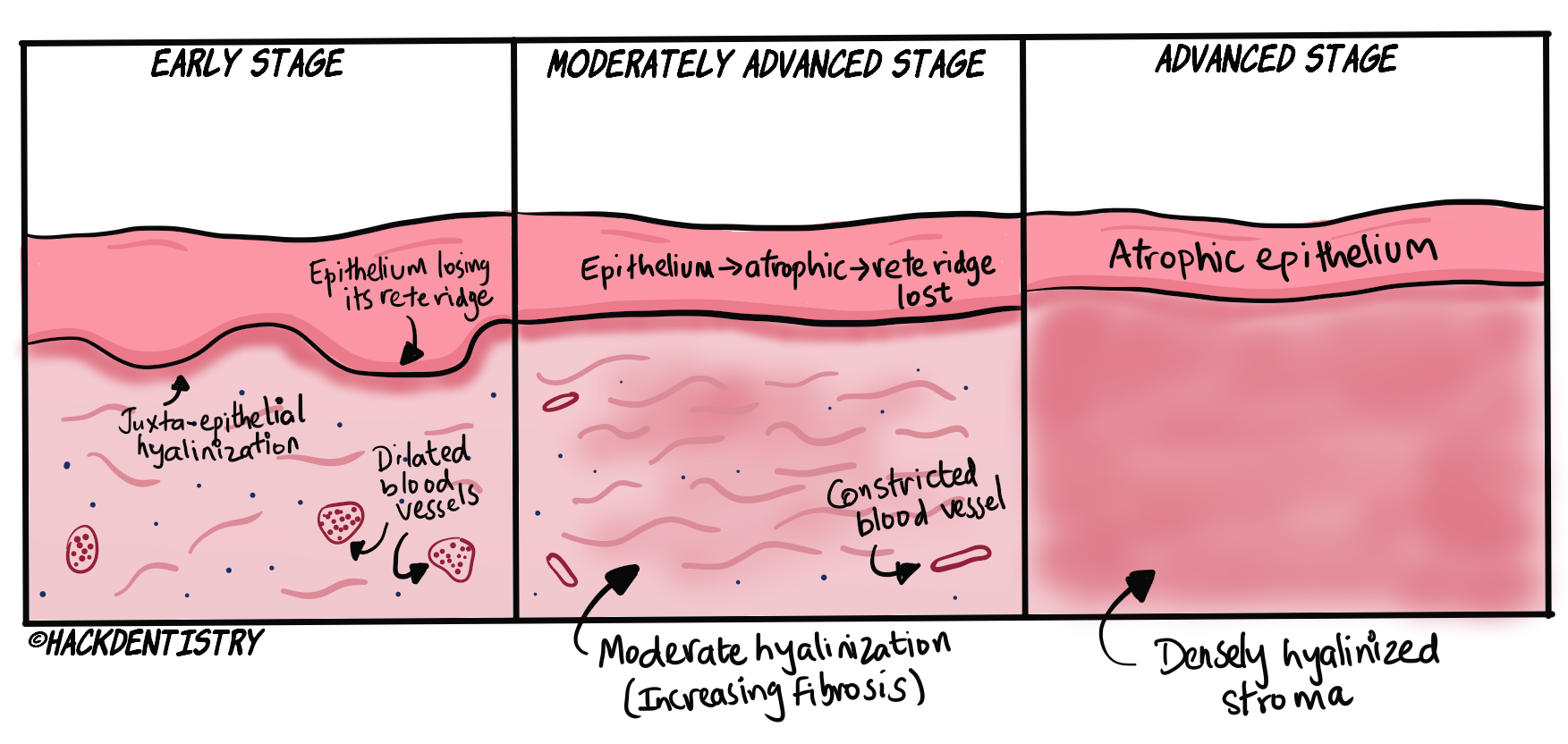
ADVANCED STAGE
Connective tissue densely fibrosed and hyalinized (appears as a smooth sheet).
Connective tissue devoid of fibroblast.
Blood vessels are obliterated.
Inflammatory infiltrate consists of lymphocytes, plasma cells and few eosinophils.
OTHER CHANGES
Epithelial dysplasia without carcinoma is found in 10-15% of cases.
OSCC is found in 5 % of cases submitted for biopsy.
TREATMENT
Intralesional injections or topical application of corticosteroids.
Hyaluronidase either topically or in combination with steroid injections are shown to improve symptoms faster and have better long term results.
Nutritional supplements like multivitamins and antioxidants improve symptoms.
Surgical excision of the fibrotic bands and laser fibrotomy could be useful in managing oral submucous fibrosis.
✅HIGHLIGHTS - VIVA & ENTRANCE EXAM PERSPECTIVE
OSF is a condition characterized by an altered collagen metabolism which results in dense fibrosis of the oral cavity.
The dense fibrosis caused in this condition is due to the presence of arecanut in betel quid.
Arecoline could upregulate the production of growth factors which cause fibroblast to increase collagen production.
Tannins (polyphenol) and copper in arecanut cause an increase in enzyme, lysyl oxidase --> causes abnormal cross-linking of collagen molecules --> decreased degradation of collagen.
Blanching starts from the lips or buccal mucosa and proceeds backwards.
Fibrous bands can be palpated (in tissues affected), usually running vertically.
OSF is classified as a potentially malignant disorder and is estimated to have a 7-13% rate of malignant transformation to oral squamous cell carcinoma (OSCC).
Early stage OSF - Juxta-epithelial hyalinization --> glassy, homogenous eosinophilic material deposited in connective tissue immediately below epithelium.
Advanced stage OSF - Connective tissue densely fibrosed and hyalinized (appears as a smooth sheet).
Hyaluronidase either topically or in combination with steroid injections are shown to improve symptoms faster and have better long term results.
QUESTIONS? BRING 'EM ON!!
As OSF progresses, it is noted (under the microscope) that the blood vessels begin to constrict and are obliterated in advanced stages. a) Why does this happen? b) Does this have any effect?
OSF can regress and oral mucosa could return to normalcy on quitting adverse habits – betel quid/arecanut chewing. Is this true?
ANSWERS
a) Progressive fibrosis of the connective tissue in OSF could cause obliteration of blood vessels and reduction in vascularity. Also there are studies reporting arecoline to possibly have cytotoxic effects on endothelial cells leading to impairment of vascular function.
b) The hypoxic environment due to reduced vascularity is one of the many reasons OSF can progress to malignancy.
No, OSF unfortunately is irreversible, and reduction or stopping the habit completely can at best slow the progress of the disease (if detected in early stages). Quitting the adverse habit is an important preventive measure. Treatment for OSF is symptomatic.
📖REFERENCES AND FURTHER READING
Ekanayaka RP, Tilakaratne WM (2013) Oral Submucous Fibrosis: Review on Mechanisms of Pathogenesis and Malignant Transformation.J Carcinogene Mutagene S5: 002.
Wollina U, Verma SB, Ali FM, Patil K. Oral submucous fibrosis: an update. Clin Cosmet Investig Dermatol. 2015;8:193–20.
Neville BW, Damm DD, Allen CM, Chi A. Oral and Maxillofacial Pathology. South Asian ed. Elsevier; 2016.
Rajendran R, Sivapathasundaram B. Shafer’s Textbook of Oral Pathology. 7th ed. Elsevier; 2012.
Regezzi JA, Sciubba JJ, Jordan RCK. Oral Pathology: Clinical Pathologic Correlations. 5 th ed. Elsevier; 2007.
Lountzis NI, Ferringer T, Macaron N, Howard A. Oral Submucous Fibrosis. 2016. Available at https://emedicine.medscape.com/article/1077241-overview