
Paget's Disease of Bone

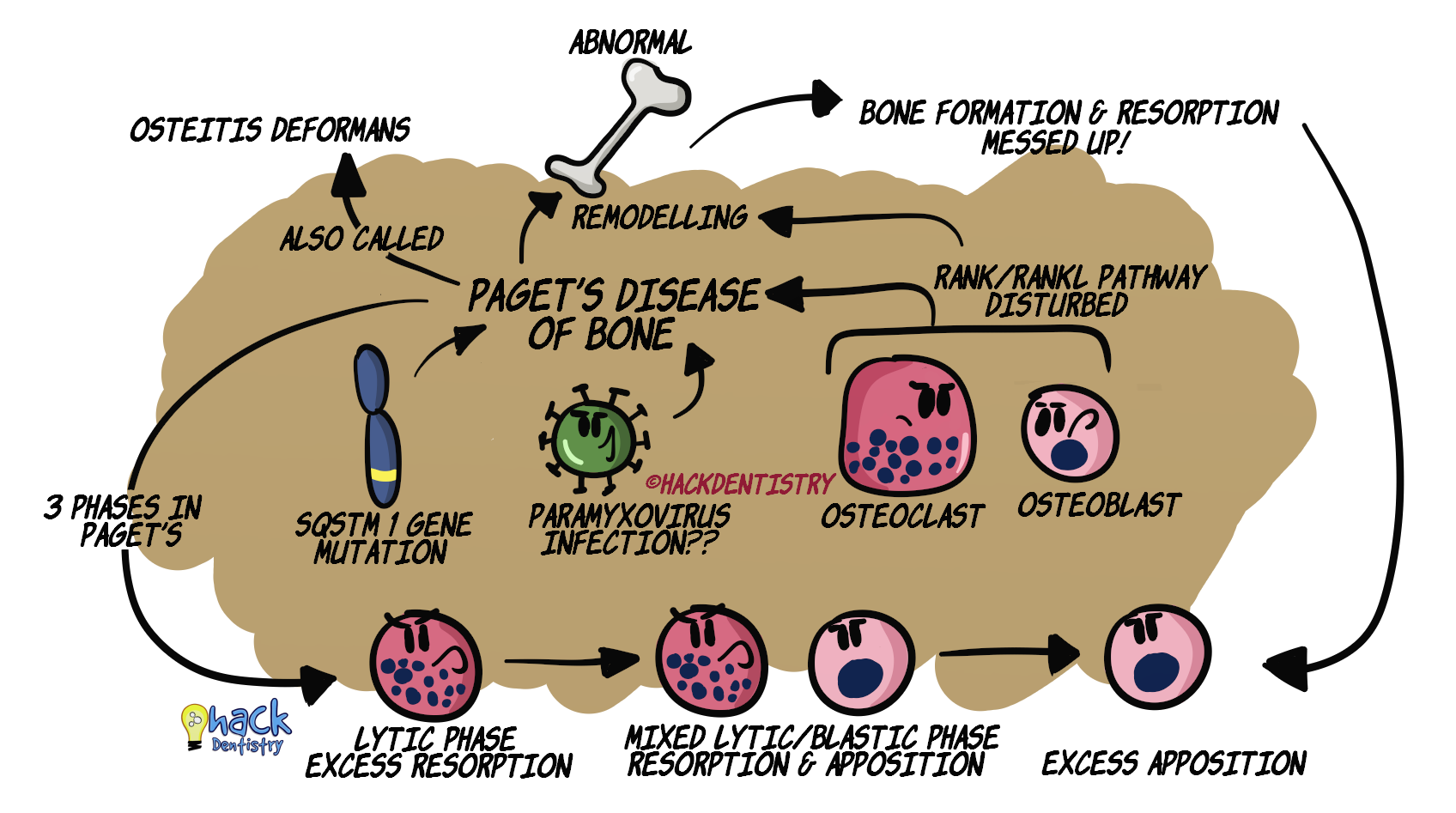
Paget’s disease of bone also called osteitis deformans is a slowly progressive metabolic bone disease.
There is an uncoordinated and simultaneous increase in bone resorption and formation/apposition.
This excessive and abnormal remodelling leads to enlarged and weak bones.
Paget’s disease is known to be the 2nd most common metabolic bone disease after osteoporosis
ETIOLOGY & PATHOGENESIS
GENETIC FACTORS
Many cases of Paget’s disease are known to be genetic, with mutated genes being present in family members.
The most well recognized gene mutations are the ones in the SQSTM1 (Sequestome 1) gene.
ENVIRONMENTAL FACTORS - VIRAL INFECTION
A controversial and unclear environmental factor proposed to cause the disease is paramyxovirus infection.
Intra-nuclear viral inclusion bodies have been identified in the lesional osteoclasts.
PATHOGENESIS
Whatever be the cause for the disease, the RANK & RANKL pathway for osteoclast formation is disturbed.
This leads to excess resorption or too little resorption of bone.
There is excess RANKL, and osteoclasts are hyper-responsive to RANKL.
There is increased IL-6 that can cause an increased osteoclastic activity.
💡Phases of Paget’s Disease
Lytic phase --> initial osteoclastic phase where there is excess bone resorption.
Mixed lytic and blastic phase --> beginning of simultaneous bone formation along with bone resorption.
Blastic/sclerotic phase --> excessive (disorganized) bone formation.
It has to be understood that, bone formation following resorption is so rapid that collagen in the organic matrix of bone is not laid out in an orderly fashion and is disorganized. So, although there are large volumes of bone deposited, it is weak and prone to pathologic fractures.CLINICAL FEATURES
GENERAL MANIFESTATIONS
Usually affects older people (>50 years); not seen in individuals below 20 years.
Paget’s disease has a male predilection.
The condition can affect a single bone (monostotic) or multiple bones (polyostotic).
Bones most affected --> pelvis, spine, femur, tibia, skull.
Patients with the disease could be asymptomatic; diagnosed during radiographic examinations or other lab tests (increased alkaline phosphatase).
Usually 50% or more patients suffering from this condition present with a dull constant, deep aching pain (in the region of the affected bone).
The pain though constant, may worsen at night.
Bone manifestations --> pain, enlargement, bowing of weight bearing bones (legs), arthritis, pathologic fractures.
Elevated skin temperature (above affected bone) --> due to bone hypervascularity.
Neurologic symptoms due to skull enlargement --> headache, deafness, impaired hearing and sight.
JAW/ORAL MANIFESTATIONS
It is estimated that 17% of patients may have jaw involvement.
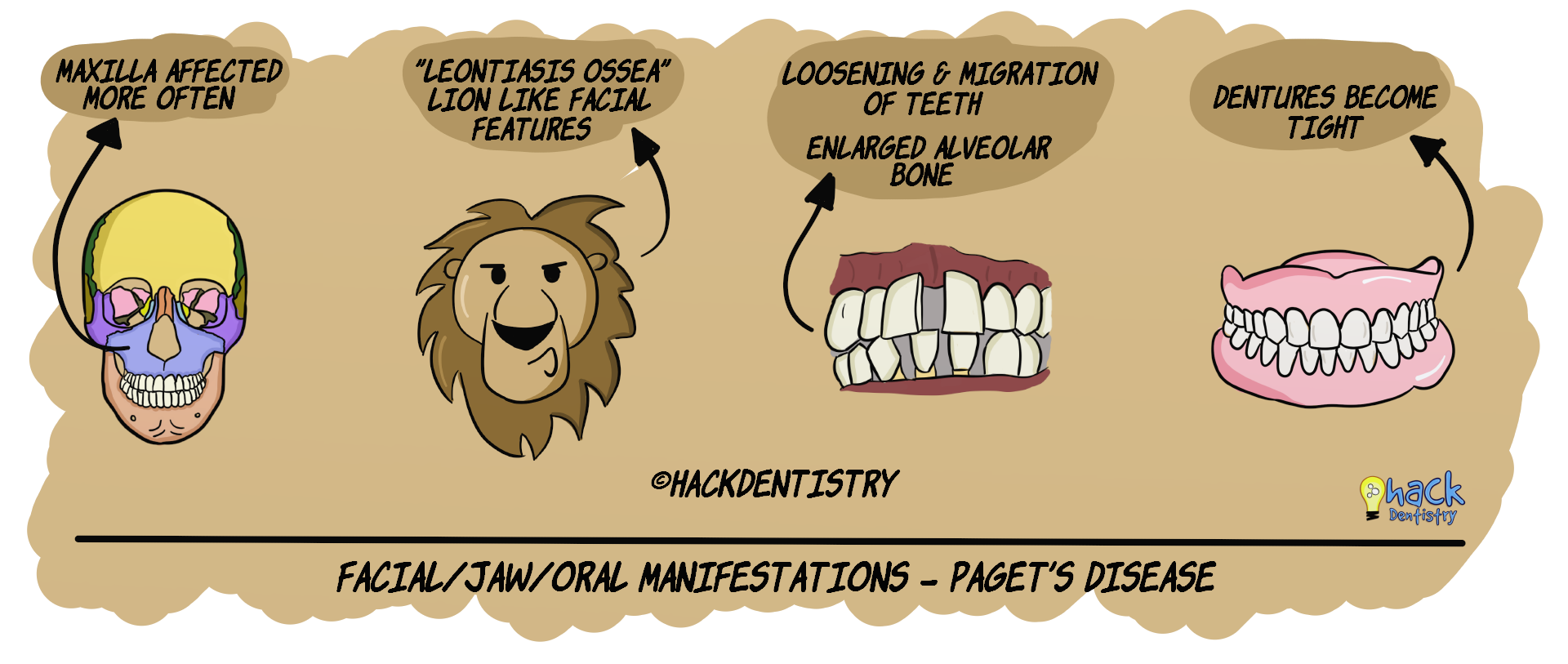
Maxilla is affected twice as much as the mandible.
Both maxillary and mandibular involvement results in jaw enlargement and facial deformity.
In addition, maxillary involvement may cause --> nasal obstruction and sinus obliteration.
Patients with enlarged facial bones are described as having “lion like facial features” called “leontiasis ossea”.
Enlarged alveolar ridges.
Flat palatal vault.
Loosening and migration of teeth --> spacing between teeth.
Difficulty in lip closure.
Edentulous patients complain of dentures becoming tight (due to alveolar enlargement).
💡Know Thy Facts!
There is a rare chance of Paget’s disease undergoing a malignant transformation to become osteosarcoma, fibrosarcoma or chondrosarcoma. RADIOLOGY FEATURES
Bones in the early (lytic) stages show a diffuse radiolucency.
Skull bone (when affected) may show discrete radiolucent regions referred to as “osteoporosis circumscripta”.
Blastic stages may give the bone a diffuse radiopacity.
A characteristic radiographic feature in Paget’s disease is the cotton-wool appearance of bone --> areas of patchy sclerosis (patchy radiopacity).
HISTOPATHOLOGY FEATURES
Early stages of the condition may show several large osteoclasts (often having 50-100 nuclei) resorbing bone trabeculae.
The marrow is replaced by a vascular connective tissue.
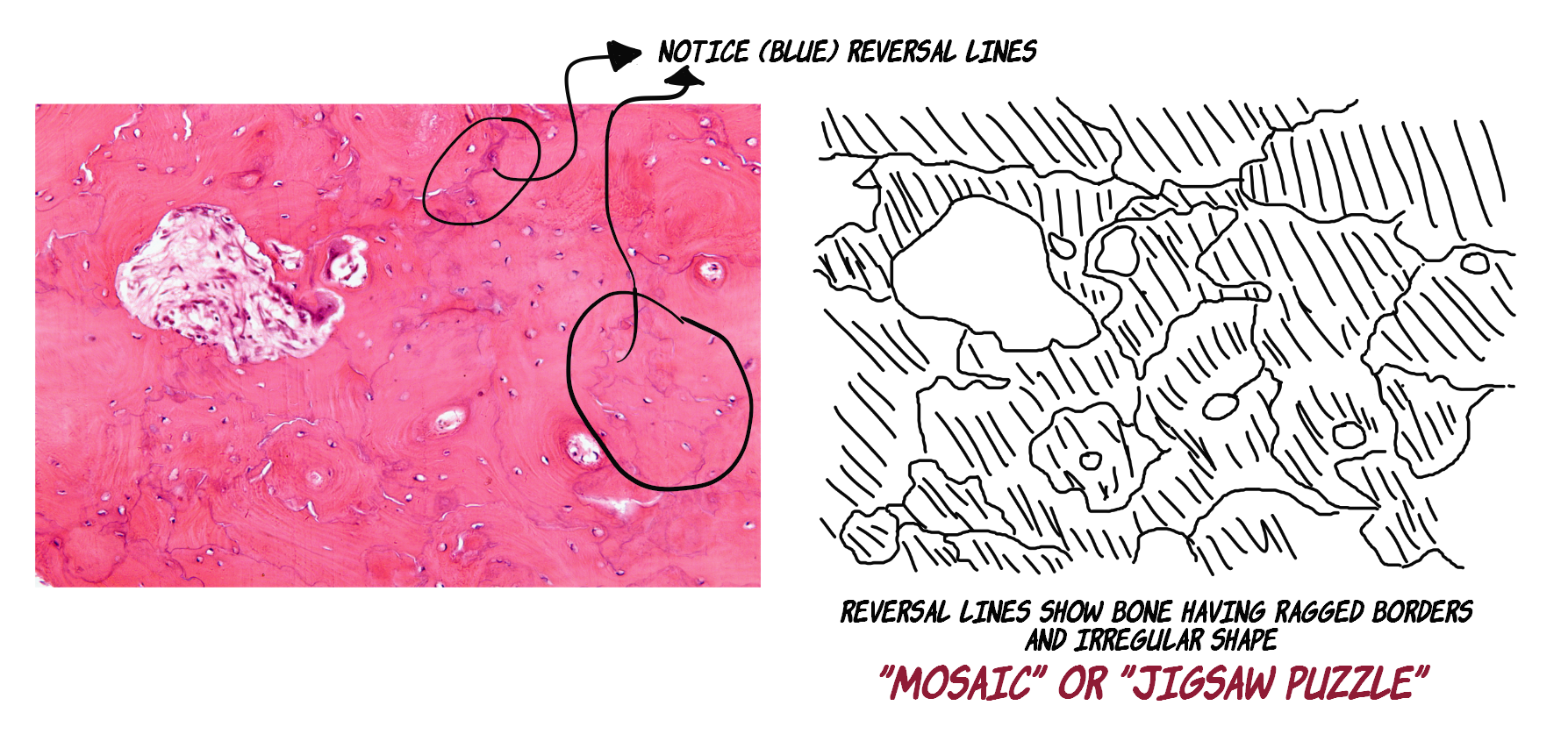
The osteoblastic stage is when the bone is being formed --> irregularly shaped new bone is deposited in areas where bone was previously resorbed. The layer between old and new one is demarcated by a “reversal line” --> gives a “mosaic” or “jigsaw puzzle appearance”.
LABORATORY FINDINGS
Normal serum calcium and phosphorus levels.
Abnormally increased serum alkaline phosphatase levels --> due to excess bone formation.
Elevated urinary hydroxylproline levels --> indicative of bone resorption.
TREATMENT
Symptomatic pain relief through analgesics.
Calcitonin or bisphosphonate therapy --> control bone resorption and apposition.
Periodic new dentures for edentulous patients.
High vascularity of bone necessitates caution during extraction or implant procedures in paget’s disease patients.
✅HIGHLIGHTS - VIVA & ENTRANCE EXAM PERSPECTIVE
Paget’s disease of bone is also called osteitis deformans.
There is an uncoordinated and simultaneous increase in bone resorption and formation/apposition.
The most well recognized gene mutations are the ones in the SQSTM1 (Sequestome 1) gene.
Paget’s disease has 3 phases in its disease course --> lytic phase, mixed lytic-blastic phase & blastic/sclerotic phase.
Bones most affected --> pelvis, spine, femur, tibia, and skull.
Usually 50% or more patients suffering from this condition present with a dull constant, deep aching pain (in the region of the affected bone).
Bone manifestations --> pain, enlargement, bowing of weight bearing bones (legs), arthritis, pathologic fractures.
Elevated skin temperature (above affected bone) --> due to bone hypervascularity.
Maxilla is affected twice as much as the mandible.
Patients with enlarged facial bones are described as having “lion like facial features” called “leontiasis ossea”.
Edentulous patients complain of dentures becoming tight (due to alveolar enlargement).
There is a rare chance of Paget’s disease undergoing a malignant transformation to become osteosarcoma, fibrosarcoma or chondrosarcoma.
Skull bone (when affected) may show discrete radiolucent regions referred to as “osteoporosis circumscripta”.
A characteristic radiographic feature in Paget’s disease is the cotton-wool appearance of bone.
Histopathology --> “mosaic” or “jigsaw puzzle appearance” of bone.
Paget’s disease may show abnormally increased serum alkaline phosphatase levels.
📖REFERENCES AND FURTHER READING
Paul Tuck S, Layfield R, Walker J, Mekkayil B, Francis R. Adult Paget's disease of bone: a review. Rheumatology (Oxford). 2017;56(12):2050-2059.
Rai NP, Anekar J, Mustafa SM, Devang Divakar D. Paget's disease with craniofacial and skeletal bone involvement. BMJ Case Rep. 2016;2016:bcr2016216173.
Shaker JL. Paget's Disease of Bone: A Review of Epidemiology, Pathophysiology and Management. Ther Adv Musculoskelet Dis. 2009;1(2):107–125.
Neville BW, Damm DD, Allen CM, Chi A. Oral and Maxillofacial Pathology. South Asian ed. Elsevier; 2016.
Regezzi JA, Sciubba JJ, Jordan RCK. Oral Pathology: Clinical Pathologic Correlations. 5 th ed. Elsevier; 2007.
Rajendran R, Sivapathasundaram B. Shafer’s Textbook of Oral Pathology. 7th ed. Elsevier; 2012.
Sapp JP, Eversole LR, Wysocki GP. Contemporary Oral and Maxillofacial Pathology. 2 nd ed. Mosby; 2004.
PICTURE ATTRIBUTION
Histopathology picture - Nephron - CC BY-SA 3.0, https://commons.wikimedia.org /w/index.php?curid = 12440623 (picture modified BY HackDentistry)