
Radicular/Periapical cyst (Note and Video)

Radicular/periapical cyst is the most common odontogenic cyst and represents 50-60% of all jaw cysts.
This cyst is inflammatory in origin. It is believed to develop from proliferating rests of Malassez in the periapical region.
Radicular cyst usually occurs in the periapical region as a sequel to dental caries causing pulpal necrosis. It could also arise as a result of tooth fracture causing necrosis of the pulp.
The cyst may be sometimes found on the lateral aspects of the roots in relation to lateral accessory root canals – called lateral radicular cyst.
PATHOGENESIS
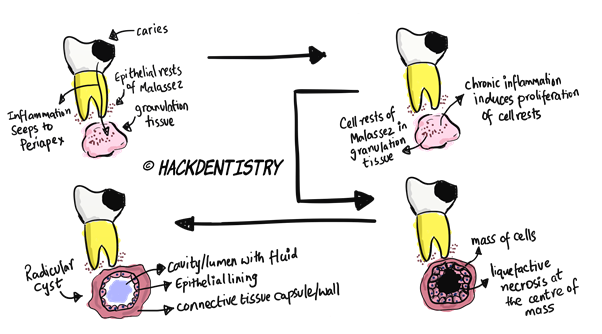
When infection (from the carious tooth) seeps through to the periapical region from an overlying tooth, a mass of reparative granulation tissue forms (provided the infection is chronic) as a defensive reaction to this microbial infection. This is called a periapical granuloma.
The chronic inflammation may induce proliferation of the rests of Malassez in the periapical granuloma (initiation phase).
A mass of cells is formed as a result of this proliferation. However, the cells at the centre of this mass do not receive nutrition and undergo liquefactive necrosis (cyst formation phase). This forms a cavity at the centre filled with fluid and lined with cells at the periphery.
The cyst may then expand by osmosis and bone resorption (expansion phase).
The most popular theory of cyst formation phase is that (the one explained above)
- Cells (of Malassez) proliferate --> form a mass of cells -> cells in the centre are away from the nutrients provided by the connective tissue --> undergo ischaemic liquefactive necrosis. This creates a central cavity surrounded by a viable epithelium.
However, there are also other schools of thought (refer video, refer reference quoted)
- Degeneration of the central cells (in the proliferated mass of cells)--> due to an immunologic reaction or autolysis (as opposed to ischaemic necrosis due to lack of nutrients). Such degenerations happen in the epithelial islands (proliferated masses of cells) in different parts of the connective tissue and may coalesce to form a larger (single) cavity!
You could refer the chapter on “Radicular cyst” in the book “Shear M, Speight PM. Cysts of the Oral and Maxillofacial Regions. 4th ed. Blackwell Munksgaard; 2007” for further details.CLINICAL FEATURES
Radicular cysts may occur at any age but appears to occur more often in people aged 30 to 60 years.
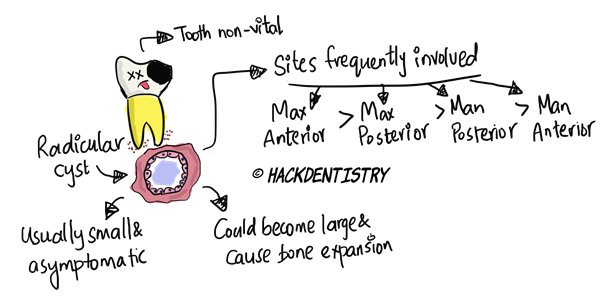
Frequency of sites involved maxillary anteriors > maxillary posteriors > mandibular posteriors > mandibular anteriors.
Very seldom are deciduous teeth involved.
Involved or associated tooth is non-vital and does to respond to vitality tests.
Radicular cysts are usually small and asymptomatic; they may be rarely painful and large causing bony expansion.
RADIOLOGY FEATURES
Radicular cyst shows a round to ovoid radiolucency with a well corticated radiopaque rim.
Associated tooth shows a loss of lamina dura.
There may be resorption of roots of associated and adjacent teeth.
It is not possible to differentiate between a radicular cyst and periapical granuloma radiographically (though a radicular cyst is usually bigger than a periapical granuloma).
HISTOPATHOLOGY FEATURES
The epithelial lining:
is stratified squamous and of variable thickness, usually 6-20 cell layers thick.
is proliferative and may show an arcading pattern.
may also, not show arcading in focal areas and may be simple stratified squamous.
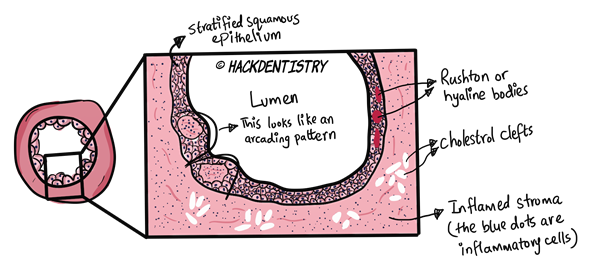
Rushton bodies or hyaline bodies are eosinophilic structures found rarely in the epithelium. These structures may be linear, concentric, curved or hairpin shaped.
The radicular cyst usually shows a moderately to severely inflamed connective tissue having lymphocytes plasma cells and macrophages.
Many radicular cysts show focal areas of numerous clefts called cholesterol clefts in the connective tissue.
TREATMENT
A thorough root canal therapy of the associated tooth.
Extraction of the tooth with curettage of the periapical tissue.
If the size of the lesion is too big for conventional endodontic therapy, an endodontic surgery is performed and the cyst removed.
✅HIGHLIGHTS - VIVA & ENTRANCE EXAM PERSPECTIVE
Radicular/periapical cyst is the most common odontogenic cyst and represents 50-60% of all jaw cysts.
This cyst is inflammatory in origin. It is believed to develop from proliferating rests of Malassez in the periapical region.
Frequency of sites involved maxillary anteriors > maxillary posteriors > mandibular posteriors > mandibular anteriors.
Involved or associated tooth is non-vital and does to respond to vitality tests.
It is not possible to differentiate between a radicular cyst and periapical granuloma radiographically.
The epithelium is proliferative and may show an arcading pattern (histopathology).
Rushton bodies or hyaline bodies are eosinophilic structures found rarely in the epithelium.
Rushton bodies or hyaline bodies are eosinophilic structures found rarely in the epithelium. These structures may be linear, concentric, curved or hairpin shaped.
QUESTIONS? BRING 'EM ON!!
What is an “apical pocket cyst”? Is it the same as a “bay cyst”?
Answer
Based on the relationship a radicular cyst shares with its associated tooth, there are two types of radicular cysts.
One type has a lumen or a cavity totally enclosed by the epithelial lining and this type is called the “apical true cyst”. This type is self-sustaining and could continue to grow if not curetted thoroughly.
The second type has its lumen or cavity in continuity with the root canal. That is, this cyst has its epithelium attached with the root apex, and is continuous with the root canal through its open lumen. This type is called the “apical pocket cyst” or “bay cyst”. Since this cyst is open it continues to grow, as long as bacteria and necrotic debris continue to seep through the canal and would definitely regress/disappear on extracting or endodontically treating the tooth.
Is there any other theory explaining the formation of radicular cyst (other than the one explained above)?
The initiation phase is followed by the cyst formation phase.
The most popular theory of cyst formation phase is that
Cells (of Malassez) proliferate --> form a mass of cells -> cells in the centre are away from the nutrients provided by the connective tissue --> undergo ischaemic liquefactive necrosis. This creates a central cavity surrounded by a viable epithelium.
However, there are also other schools of thought
Degeneration of the central cells (in the proliferated mass of cells)--> due to an immunologic reaction or autolysis (as opposed to ischaemic necrosis due to lack of nutrients). Such degenerations happen in the epithelial islands (proliferated masses of cells) in different parts of the connective tissue and may coalesce to form a larger (single) cavity!
You could refer the chapter on “Radicular cyst” in the book “Shear M, Speight PM. Cysts of the Oral and Maxillofacial Regions. 4th ed. Blackwell Munksgaard; 2007” for further details.
Why do you think there may be cholesterol clefts formed in the connective tissue?
Answer
Cholesterol clefts are formed due to accumulation of cholesterol in the connective tissue, which then gets dissolved out during histologic preparations forming clefts. These cholesterol accumulations are hypothesized to be derived from the cell walls of disintegrating red blood cells, lymphocytes, plasma cells and macrophages.
📖REFERENCES AND FURTHER READING
Shear M, Speight PM. Cysts of the Oral and Maxillofacial Regions. 4 th ed. Blackwell Munksgaard; 2007.
Neville BW, Damm DD, Allen CM, Chi A. Oral and Maxillofacial Pathology. South Asian ed. Elsevier; 2016.
Rajendran R, Sivapathasundaram B. Shafer’s Textbook of Oral Pathology. 7th ed. Elsevier; 2012.
Regezzi JA, Sciubba JJ, Jordan RCK. Oral Pathology: Clinical Pathologic Correlations. 5 th ed. Elsevier; 2007.
Sapp JP, Eversole LR, Wysocki GP. Contemporary Oral and Maxillofacial Pathology. 2 nd ed. Mosby; 2004.