
Tobacco pouch keratosis (Note & Video)

Tobacco pouch keratosis (TPK) is also synonymously called snuff dipper’s lesion and smokeless tobacco keratosis.
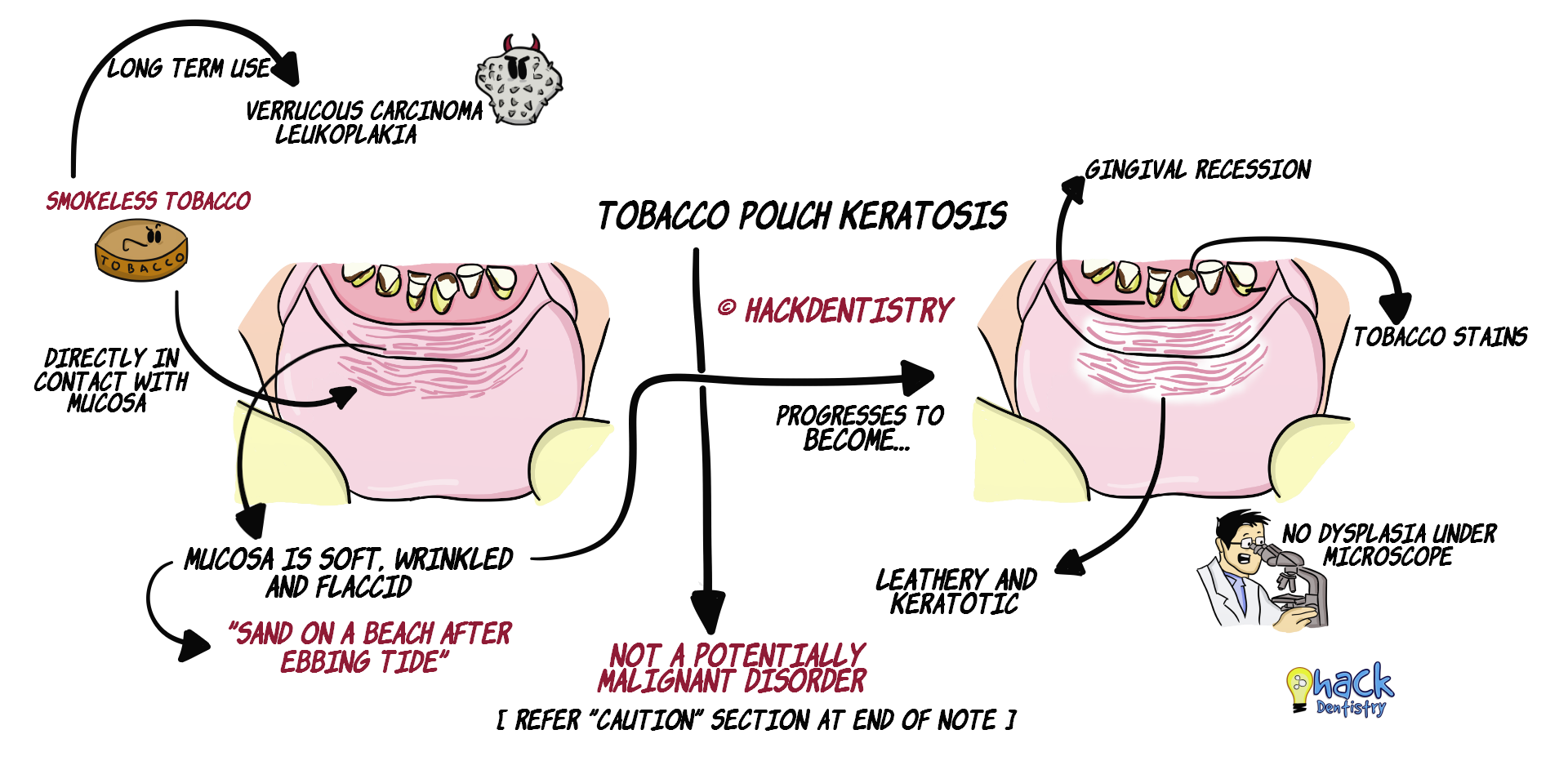
TPK, as the name implies is a white keratotic lesion that appears in the mucosa due to a chronic smokeless tobacco habit. The affected mucosa is pouch-like because it becomes soft, wrinkled and flaccid on chronic contact with tobacco.
TPK is not a potentially malignant disorder and does not show dysplasia histopathologically.
Long term usage of smokeless tobacco may however induce lesions like leukoplakia (showing dysplasia or carcinoma) and verrucous carcinoma.
ETIOLOGY
TPK is induced by chronic usage of smokeless tobacco.
Smokeless tobacco habit is prevalent among people in United States, Sweden, India and other South-East Asian countries.
Smokeless tobacco is known to have carcinogens like nitrosonornicotine.
Also its high alkalinity (8.2-9.3) along with its constant contact with the mucosa induces inflammation and a keratotic response.
💡KNOW THY FACTS!
Smokeless tobacco is available in different forms --> a) dry snuff, b) moist snuff & c) chewing tobacco. While people in the western part of the world usually use snuff, people in India and South-Asian countries mostly use chewing tobacco along with betel leaves, arecanut, lime and other spices. However, it is shredded tobacco (snuff) which has more potential to cause these lesions.CLINICAL FEATURES
TPK is prevalent among the young (adolescents/teenagers) and the older (6th decade) age group, predominantly men although certain subpopulations have older women more commonly affected.
The lesion appears in the mucosa that is directly in contact with tobacco. It is habitually placed in the mandibular vestibular area (buccal or labial).
The mucosa in individuals with TPK initially appears soft, wrinkled and granular. TPK does not have distinct borders.
The mucosa progresses to become a leathery and keratotic (white or grey coloured) with heavy folding of the mucosa.
TPK has been described as having an appearance resembling “sand on a beach after an ebbing tide”.
Pouching tobacco in the oral mucosa has also been associated with gingival recession (that gingiva in contact with tobacco).
HISTOPATHOLOGY FEATURES
Histopathology is non-specific.
Affected mucosa shows an epithelium with hyperkeratosis and acanthosis (hyperplasia of the spinous layer).
The corneal layer may sometimes have pointed projections of keratin called “chevrons”.
The upper layers of the epithelium may show intracellular edema or “vacuolization”.
The connective tissue shows sparse inflammatory infiltrate.
TPK does not show epithelial dysplasia.
TREATMENT
No treatment is required as these lesions regress in a few weeks on cessation of the habit (smokeless tobacco).
CAUTION!
TPK is a white keratotic and wrinkled lesion that resembles leukoplakia. It is important to distinguish this lesion from leukoplakia, as it usually disappears on cessation of the habit; and also does not show dysplasia histopathologically. However, if the lesion persists for at least 4-6 weeks even on cessation of the habit, the lesion could well be leukoplakia. It would be wise to take a biopsy to check for dysplastic or malignant changes.

✅HIGHLIGHTS - VIVA & ENTRANCE EXAM PERSPECTIVE
Tobacco pouch keratosis (TPK) is also synonymously called snuff dipper’s lesion and smokeless tobacco keratosis.
TPK is not a potentially malignant disorder and does not show dysplasia histopathologically.
The lesion appears in the mucosa that is directly in contact with tobacco. It is habitually placed in the mandibular vestibular area (buccal or labial).
TPK has been described as having an appearance resembling “sand on a beach after an ebbing tide”.
TPK does not show epithelial dysplasia.
If TPK persists for at least 4-6 weeks even on cessation of the habit (smokeless tobacco), the lesion could well be leukoplakia. It would be wise to take a biopsy to check for dysplastic or malignant changes.
📖REFERENCES AND FURTHER READING
Donald PM, Renjith G, Arora A. Tobacco Pouch Keratosis in a young individual: A brief description. J Indian Soc Periodontol. 2017;21(3):249–251.
Neville BW, Damm DD, Allen CM, Chi A. Oral and Maxillofacial Pathology. South Asian ed. Elsevier; 2016.
Rajendran R, Sivapathasundaram B. Shafer’s Textbook of Oral Pathology. 7th ed. Elsevier; 2012.
Regezzi JA, Sciubba JJ, Jordan RCK. Oral Pathology: Clinical Pathologic Correlations. 5 th ed. Elsevier; 2007.